By Waikeong P. Wong, MD, PhD
History
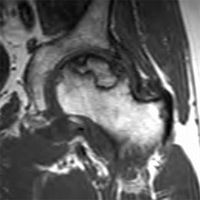
A 43-year-old man with a history of alcohol abuse, pancreatitis, and chronic liver disease presented with left hip pain.
Diagnosis
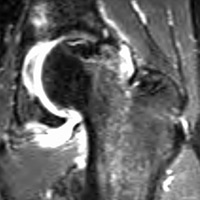
Avascular necrosis of femoral head
Clinical
• Patients may be asymptomatic early in the disease process but ultimately present with pain and limitation of motion.
• Pain is most commonly in the groin area but may also manifest in the ipsilateral buttock, knee, or greater trochanteric region.
• Pain is usually exacerbated with weight bearing and relieved with rest.
• Predisposing factors include corticosteroids, alcohol abuse, chronic liver disease, pancreatitis, coagulopathy, and hemoglobinopathies; traumatic etiologies include femoral neck fracture, hip dislocation, and slipped capital femoral epiphysis.
Key Diagnostic Features (MRI)
• MRI is the most sensitive modality and demonstrates changes well before plain film changes are visible.
• Diffuse edema
• Serpiginous low T1 signal line
• Double line sign: inner high T2 signal line representing granulation tissue and outer low signal line representing sclerotic bone at the periphery of osteonecrotic region
Differential Diagnosis
• Femoral neck stress fracture
• Synovitis
• Idiopathic transient osteoporosis of the hip
• Chondroblastoma
• Metastatic disease
Treatment
Treatment varies with location and stages of osteonecrosis: conservative (anti-inflammatory, analgesia, non-weight bearing), core decompression, and joint replacement for end-stage disease.
— Waikeong P. Wong, MD, PhD, is a radiology resident at Saint Barnabas Medical Center in Livingston, New Jersey.
 |
 |
 |
REFERENCES
- Zurlo JV. The double-line sign. Radiology. 1999; 212:541-542.
- Manaster BJ, May DA, Disler DG. Musculoskeletal Imaging. Philadelphia, PA: Mosby Elsevier; 2007.
Submission Instructions
Submit cases directly to Rahul V. Pawar, MD, DABR (section editor for “On the Case”) at rvp325@yahoo.com. Cases submitted should be relevant and interesting. All modalities and subspecialties within radiology are equally considered.
Case submission entails two PowerPoint slides:
SLIDE 1
a. History (one-line phrase)
b. Two to five high-quality images in JPEG format without annotations
c. Name(s) of the author(s) (three maximum) and respective institutions
SLIDE 2
a. Diagnosis
b. Concise bulleted discussion (one to two lines each), including the following: pertinent clinical history, diagnostic imaging findings, differential diagnoses, treatment (if applicable)
c. Two to three relevant and current references, preferably citing peer-reviewed radiology literature
Department of Radiology, Division of Neuroradiology
Saint Barnabas Medical Center/Barnabas Ambulatory Care Center