 April 2017
April 2017
On the Case
By Ryan Joyce, MD; Atul Kumar, MD; and Mark Kane, MD
Radiology Today
Vo. 18 No. 4 P. 28
History
A 30-year-old HIV-positive man presented to the emergency department (ED) after discontinuing his highly active antiretroviral therapy (HAART) medication for approximately two weeks. His chief complaint at presentation was bilateral nontender jaw swelling.
Findings
During the patient's ED course, a contrast-enhanced maxillofacial CT was performed as the initial diagnostic examination. Source axial images and reconstructed coronal and sagittal images demonstrated bilateral multiseptated mixed solid and cystic lesions scattered within the bilaterally enlarged and hyperdense parotid glands (Figures 1 and 2).
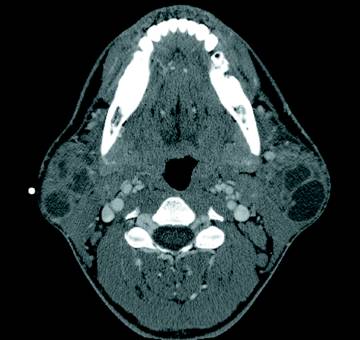
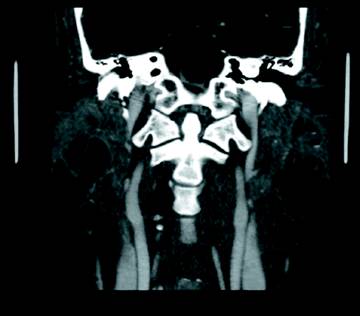
Hounsfield density of the cystic components of these parotid lesions ranged from 10 to 50. Solid and cystic lesions were not found outside of the parotid glands. There was also mild hypertrophy of the adenoid tonsils (lymphoid hyperplasia). In addition, relatively mild cervical chain lymph node enlargement was present bilaterally. Visualized lymph nodes did not meet pathologic lymphadenopathy by size criteria and were less prominent in size and extent than would be expected when considering infection or malignancy.
Diagnosis
Benign lymphoepithelial lesions (BLEL) of HIV.
Discussion
BLEL of the parotid gland is a relatively common salivary gland pathology in HIV-positive patients, with 5% of patients eventually developing BLEL. It is important to recognize that BLEL of the parotid or salivary glands may represent the first clinical manifestations of HIV infection, and they usually develop before AIDS. Clinically, patients present with relatively nontender bilateral jaw swelling in the region of the parotid glands.
The differential diagnosis for parotid lesions in HIV-positive patients includes parotitis secondary to infection, diffuse infiltrative lymphocytosis syndrome, Warthin's tumor, Sjögren's syndrome, sicca syndrome, intraparotid lymphadenopathy, Cryptococcus infection, and salivary gland neoplasms such as adenoid cystic carcinoma, Kaposi sarcoma, and lymphoma. Pathogenesis of BLEL is hypothesized to occur by one of two pathways. An "obstructive theory" states that HIV-related lymphoid hyperplasia leads to parotid/salivary ductal obstruction, and the resultant ductal dilatation produces cystic formations. The other hypothesis states that HIV-related lymphoid hyperplasia occurs within the intraparotid lymph nodes and that parotid epithelium is trapped and forms cystic formations without epithelial excretions reaching the ducts.1
On imaging, BLEL may present as multiple solid, mixed solid and cystic, or cystic intraparotid lesions. Additionally, tonsillar hyperplasia may be present, and approximately 50% of patients will have associated mild cervical lymphadenopathy. In our case, BLEL was diagnosed by the presence of bilateral parotid gland enlargement with multiple multiseptate mixed solid and cystic intraparotid lesions and mild hypertrophy of the adenoid tonsils. Ultrasound imaging can demonstrate a wide spectrum of findings, ranging from multiple intraparotid simple cysts to mixed masses with predominantly solid components. Doppler interrogation typically demonstrates heterogeneous flow patterns within the lesions.2
Importantly, malignant transformation within parotid lesions has been reported and, though uncommon, if there is concern, recent studies suggest that dynamic contrast-enhanced MRI of the parotid glands can differentiate between malignant and benign parotid lesions.3 HAART has been shown to treat BLEL with lesion resolution occurring in most patients. BLELs can reappear, as in our case, if HAART therapy is terminated.
— Ryan Joyce, MD, is a radiology resident at UConn Health, University of Connecticut.
— Atul Kumar, MD, is a radiology resident at UConn Health.
— Mark Kane, MD, is the section head for ultrasonography and an assistant professor in radiology at UConn Health.
References
1. Sujatha D, Babitha K, Prasad RS, Pai A. Parotid lymphoepithelial cysts in human immunodeficiency virus: a review. J Laryngol Otol. 2013;127(11):1046-1049.
2. Martinoli C, Pretolesi F, Del Bono V, Derchi LE, Mecca D, Chiaramondia M. Benign lymphoepithelial parotid lesions in HIV-positive patients: spectrum of findings at gray-scale and Doppler sonography. AJR Am J Roentgenol. 1995;165(4):975-979.
3. Gadodia A, Bhalla AS, Sharma R, Thakar A, Parshad R. Bilateral parotid swelling: a radiological review. Dentomaxillofac Radiol. 2011;40(7):403-414.
