 On the Case
On the Case
By Scott P. Patterson, MD; Robert E. Schilken, MD; and Richard H. Daffner, MD
Radiology Today
Vol. 19 No. 4 P. 28
History
A 30-year-old woman presented with a complaint of lateral left knee pain and swelling. She recalled simultaneously twisting and hyperextending her knee as she descended the stairs. Afterwards, she was unable to fully actively extend her knee. Physical exam revealed a small joint effusion with lateral joint line tenderness. Her anterior-posterior drawer test and varus-valgus stress test were negative. Preliminary radiographs of the knee revealed no osseous pathology. She was referred for an MRI of the left knee with a suspected lateral meniscal tear.
Findings
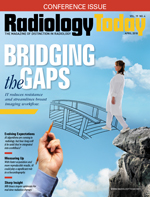
Left knee axial proton density fat saturated (Figure 1), sagittal proton density fat saturated (Figure 2), and coronal short T1 inversion recovery MRI images (Figure 3) demonstrate a diffusely thickened and edematous popliteus muscle. The proximal tendinous femoral attachment is intact. There is a small knee joint effusion. The ligamentous and meniscal structures, which are not included on the submitted images, were intact. Also, no significant osseous or cartilaginous pathology was present.
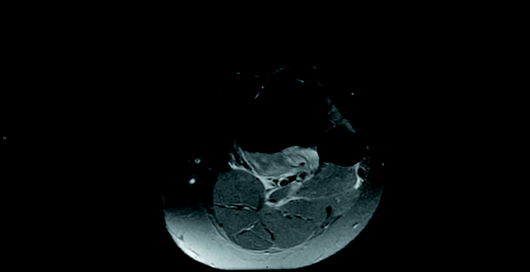
Figure 1
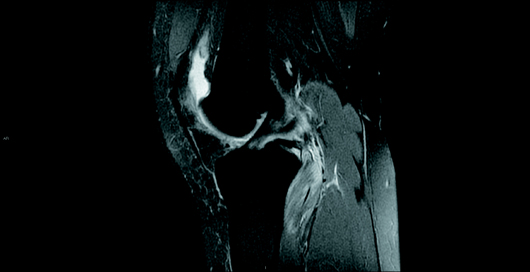
Figure 2

Figure 3
Diagnosis
Isolated intrasubstance tear of the popliteus muscle.
Discussion
The popliteus musculotendinous unit is a key static stabilizer of the posterior corner of the knee.1 The popliteus musculotendinous unit is unique in that the distal muscular attachment is designated the insertion, and the tendinous proximal femoral attachment is designated the origin.2
Various static and dynamic functions have been attributed to the popliteus, including "unlocking" of the knee joint, initiation and maintenance of internal rotation of the tibia on the femur, and preventing forward dislocation of the femur on the tibia during initial flexion.3 The popliteus, although small, is the only muscle that has sufficient mechanical advantage to produce internal rotation of the tibia on the femur during gait.4
Isolated injuries to the popliteus musculotendinous unit are rare, and few cases are described in the literature. Popliteus muscle and tendon injuries are usually associated with posterior lateral corner injuries of the knee. In these cases, the injury is extensive and may include disruption of the arcuate ligament complex, the lateral collateral ligament, both cruciate ligaments, and the menisci.5 According to one study, less than 10% of popliteus injuries are isolated, and they usually occur in the setting of significant trauma.3
The clinical history is often misleading and may lead to an incorrect preliminary diagnosis.2 Various mechanisms of injury to the popliteus muscle have been described. The most common is a combined hyperextension with an external tibial rotational force.3 As in this case, clinical history and physical examination usually suggest an alternative presumed diagnosis such as a cruciate ligament or meniscal tear. Other pathologies in the differential diagnosis that may cause similar symptoms include osteochondritis dissecans, iliotibial band tendonitis, and popliteal cyst.6 In the presence of ligamentous stability and an intact popliteus tendon, patients with interstitial muscle tears respond well to conservative management, as demonstrated in this case.1,5,6
On her return visit 11 days after the initial encounter, the patient reported significant improvement in symptoms. The patient's injury was treated conservatively with limited weight-bearing and nonsteroidal anti-inflammatory drug therapy. After the imaging findings were reviewed, she was referred to physical therapy in order to undergo a strengthening program.
— Scott P. Patterson, MD, is director of MRI and a staff radiologist at St. Clair Hospital in Pittsburgh.
— Robert E. Schilken, MD, is an orthopedic surgeon with the Allegheny Health Network and a clinical instructor at the Drexel University College of Medicine in Pittsburgh.
— Richard H. Daffner, MD, is emeritus professor of radiology at Temple University School of Medicine, Allegheny Campus in Pittsburgh.
References
1. Guha AR, Gorgees KA, Walker DI. Popliteus tendon rupture: a case report and review of the literature. Br J Sports Med. 2003;37(4):358-360.
2. Burstein DB, Fischer DA. Case report: isolated rupture of the popliteus tendon in a professional athlete. Arthroscopy. 1990;6(3):238-241.
3. UW MSK resident projects: popliteus muscle injury. University of Washington, UW MSK Radiology Web Lab website. uwmsk.org/residentprojects/popliteus.html. Published August 7, 2003.
4. Barnett CH, Richardson AT. The postural function of the popliteus muscle. Ann Phys Med. 1953;1(5):177-179.
5. Doucet C, Gotra A, Reddy SMV, Boily M. Acute calcific tendinopathy of the popliteus tendon: a rare case diagnosed using a multimodality imaging approach and treated conservatively. Skeletal Radiol. 2017;46(7):1003-1006.
6. Jadhav SP, More SR, Riascos RF, Lemos DF, Swischuk LE. Comprehensive review of the anatomy, function, and imaging of the popliteus and associated pathologic conditions. Radiographics. 2014;34(2):496-513.