 On the Case
On the Case
By Pramod Gupta, MD, and Francisco Garcia-Morales, MD
Radiology Today
Vol. 18 No. 12 P. 28
History
A 40-year-old man with a complicated cardiac history was admitted for elective mitral valve clipping to treat severe mitral regurgitation. The patient had a history of hypertension and had an acute myocardial infarction nine years prior, for which he had a percutaneous cardiac intervention (PCI) with two Cypher stents—drug-eluting coronary stents from the Cordis Corporation—placed in the right coronary artery (RCA). Subsequently, he developed ischemic cardiomyopathy and severe mitral regurgitation. He had another acute myocardial infarction event three years prior and had balloon angioplasty of in-stent stenosis of the RCA with additional placement of two overlapping zotarolimus-eluting stents. During the current admission for mitral valve clipping, transesophageal echocardiogram showed an echogenic linear structure in the ascending aorta originating from the RCA. A dislodged coronary stent was suspected; coronary CT angiogram (CTA) was performed.
Findings
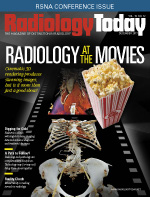
Long and short axis transesophageal echocardiogram images demonstrate an echogenic linear structure in the ascending aorta originating from the right coronary cusp (Figures 1 and 2). Sagittal oblique, sagittal, and short axis CTA images show a long segment of the RCA stent in the ascending aorta, one end freely floating and another end wedged at the right coronary ostium (Figures 3, 4, and 5).

Figure 1
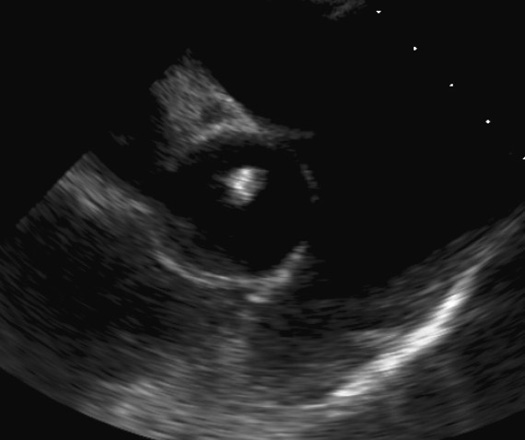
Figure 2
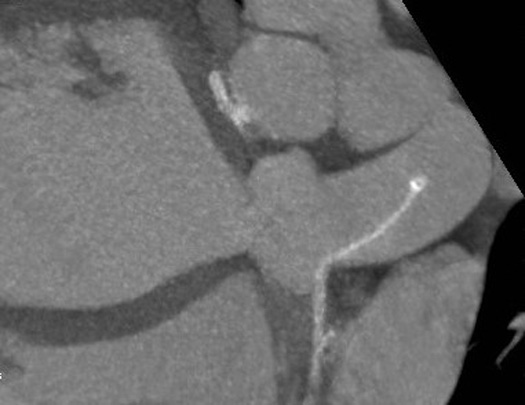
Figure 3
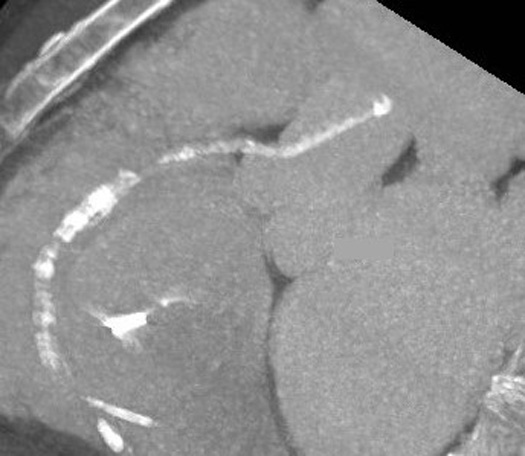
Figure 4

Figure 5
Diagnosis
Coronary artery stent dislodgement into the ascending aorta.
Discussion
Stent dislodgement is a rare and potentially life-threatening complication of PCI. Complications can include stent and artery thrombosis and stent embolization. Factors that may predispose a patient to stent dislodgement are poor support to a guiding catheter or guide wire, vessel tortuosity, inadequate predilatation, vessel calcification, and a preexisting stent. It was not clear in this patient whether the stent dislodgement happened at the time of PCI three years prior and went undetected or happened over time.
Although the most desirable treatment is to remove the stent, this is not always feasible. Several percutaneous and surgical methods of retrieving dislodged stents from the coronary artery have been described, including myocardial biopsy, double-wire braiding technique, multipurpose baskets, loop snares, small-balloon technique, and stent-crush exclusion technique. In this patient, considering the high risk associated with percutaneous or surgical removal of the stent without avoiding RCA injury, it was decided to treat the patient with dual antiplatelet therapy to maintain RCA patency.
— Pramod Gupta, MD, is a staff radiologist at the Dallas VA Medical Center.
— Francisco Garcia-Morales, MD, is a staff radiologist at the Dallas VA Medical Center.
Resources
1. Porwal SC, Halkati PC, Patted SV, Joshi A. Successful deployment of a dislodged sirolimus-eluting stent with a small-balloon technique. J Cardiol Cases. 2013;8:155-157.
2. Yang DH, Woo SI, Kim DH, et al. Two dislodged and crushed coronary stents: treatment of two simultaneously dislodged stents using crushing techniques. Korean J Intern Med. 2013;28(6):718-723.
3. Tekleyes FG, Lester MD, Studeny MA, Thompson EA, Craig S. An unusual migration of a stent: a case reort. Marshall J Med. 2016;2(2):31-36.
