 On the Case
On the Case
By Paola Tabaro, MD; Michelle Romero, MD; and Alex Merkulov, MD
Radiology Today
Vol. 23 No. 6 P. 38
History
A 35-year-old man with a past medical history of alcohol use disorder, hypertension, and osteonecrosis of the right hip presented to the emergency department with headaches, confusion, and word-finding difficulty. A high-grade fever of 102° F was present at that time. CT of the brain was performed with findings suspicious of viral encephalitis. A lumbar puncture showed elevated protein (445) and white blood cells (693) with mononuclear cell predominance, three red blood cells, and normal glucose. The patient was admitted for herpes encephalitis and started on ceftriaxone, vancomycin, and acyclovir. (His partner was found to be herpes positive). Two days later, the patient’s mental status worsened, and he became more confused. Repeat imaging of the brain with CT and MRI showed extensive edema in the left temporal lobe with petechial hemorrhage and a 7-mm left-to-right midline shift. The patient was also becoming bradycardic to the 40s. Neurosurgery was consulted, and the patient underwent a decompressive hemicraniectomy for left temporal lobe ischemic stroke with brain stem compression (secondary to uncal herniation) and cerebral edema causing herniation syndrome (right upper extremity and face weakness and worsening aphasia) and a left temporal lobe biopsy.
Findings
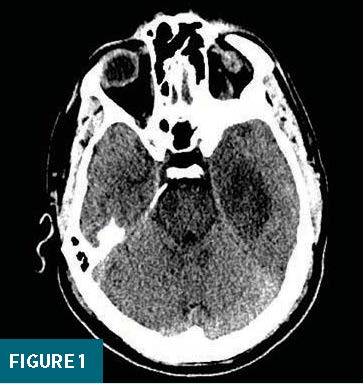
Initial noncontract CT of the brain showed a hypodensity in the left medial temporal lobe, without evidence of hemorrhage (Figure 1).
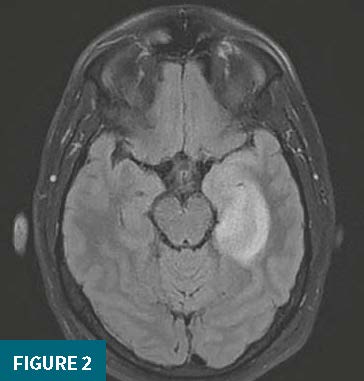
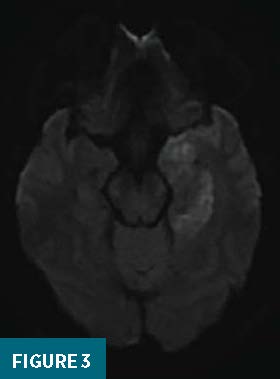
Concurrent MRI without and with IV contrast demonstrated abnormal localized T2 fluid-attenuated inversion recovery (FLAIR) hyperintensity in the inferomedial left temporal lobe (Figure 2) with associated high signal intensity on diffusion-weighted imaging (DWI) (Figure 3). Mild diffuse enhancement in the inferomedial aspect of the left temporal lobe was also noted. There was sparing of the basal ganglia.
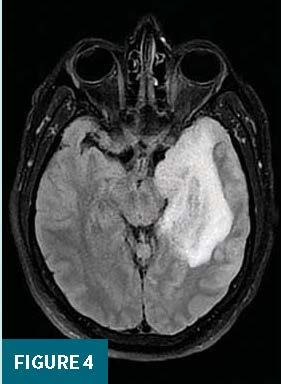
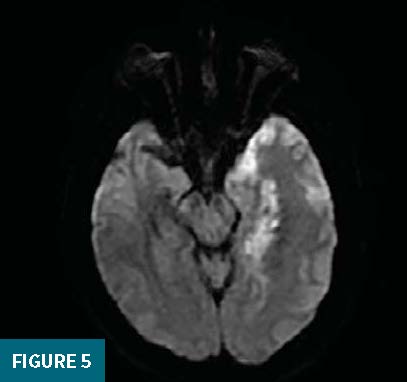
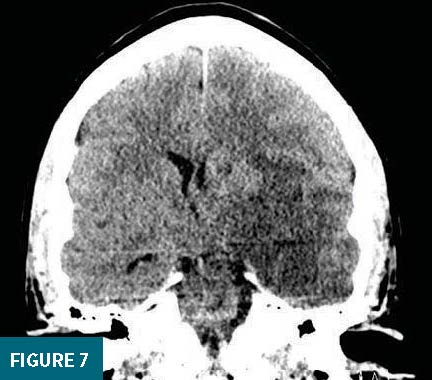
Follow up imaging, performed three days later secondary to worsening clinical symptoms, showed significantly increased left temporal lobe T2 FLAIR hyperintense signal extending posteriorly into the occipital lobe (Figure 4) and superiorly into the insular cortex and increased area of restricted diffusion on DWI (Figure 5). A 7-mm left-to-right midline shift (Figures 6 and 7) and a prominent left hyperdense middle cerebral artery was noted on CT. Findings were compatible with superimposed acute ischemic infarction involving the medial temporal and occipital lobes. Additional CT angiograms of the head and neck were normal without evidence of a large vessel occlusion.
After a lengthy course in the intensive care unit, the patient was eventually discharged home. On follow-up with neurology, the patient has residual facial paresthesias and a few breakthrough seizures.

Diagnosis
Encephalitis due to human herpes simplex virus (HSV).
Discussion
Infectious etiologies account for nearly 50% of reported encephalitis cases. HSV is the most frequently identified cause of encephalitis in developed countries, approximately accounting for 30% to 50% of reported cases.1
Two subtypes of HSV encephalitis are recognized, which differ in demographics, virus, and pattern of involvement. They are neonatal herpes encephalitis and childhood and adult herpes encephalitis.
The herpes virus family is double-stranded DNA viruses that establish lifelong infection once they invade their host, known for their rapid spread among individuals. HSV initially gains access to the host through mucous membranes or damaged skin barriers.2 Herpes encephalitis is caused by HSV-1 type, which is associated with oropharyngeal and mucosal infections in children. It is thought that after primary infection, the virus travels to neuronal cell bodies in the dorsal root ganglion via retrograde axonal transport and can remain dormant for years. The exact mechanism of how HSV enters the central nervous system is not well understood, but past research studies have proposed that the most likely routes of transport include transport through the olfactory or trigeminal nerves, which explains the predilection of HSV-1 for the frontal and mesiotemporal lobes.1
It is unknown whether HSV encephalitis starts as a reactivation of a latent virus in the trigeminal ganglia or as a primary infection. Reactivation may occur spontaneously or be precipitated by various factors, such as trauma, immunosuppression, hormonal fluctuations, or emotional stress. Once active infection with HSV occurs, a massive immune response is triggered to clear the active infection leading to necrosis and apoptosis of infected cells and a subsequent inflammatory response that contributes to local tissue destruction.1
Most patients present with altered mental status, fevers, and symptoms of brain inflammation such as seizures and headaches. A prodrome of upper respiratory tract infections has also been reported.3 Final diagnosis is established with a polymerase chain reaction of cerebrospinal fluid, although the combination of the clinical symptoms, cerebrospinal fluid demonstrating pleocytosis and elevated protein, and positive imaging findings is sufficient to start treatment.1
It is essential to appropriately diagnose and start early treatment for HSV encephalitis to improve morbidity and mortality. HSV encephalitis has a 50% to 70% mortality rate, and rapid diagnosis can improve outcomes.3 Common complications of HSV encephalitis include cerebral edema, hemorrhage, infarction, and herniation.1
HSV encephalitis mainly affects the anterior and medial temporal lobes, insular cortex, subfrontal area, cingulate gyrus, and thalami in an asymmetric unilateral or bilateral distribution.4
MRI with and without contrast is the preferred imaging modality for encephalitis. Imaging findings include asymmetric hyperintense foci on T2 and FLAIR, which correspond to areas of edema with a predilection for the mesiotemporal and orbitofrontal lobes.4 On postcontrast TI DWI, patchy areas of parenchymal and leptomeningeal enhancement can be seen. In the early disease course, restricted diffusion representing cytotoxic edema may be the first finding and can sometimes precede changes on T2 or FLAIR imaging.1 Contrary to popular belief, hemorrhage is rarely noted but, if present, will show blooming artifact on gradient echo sequences.2 Nonenhanced CT imaging can be normal in the early disease course or present as a focal, asymmetric, low attenuating area with mild mass effect in the typical locations for HSV encephalitis.1 Contrast-enhanced CT imaging can demonstrate patchy or gyriform enhancement within the temporal lobe.2 Pathologic examination usually shows diffuse leptomeningeal and parenchymal inflammation, which can lead to hemorrhage and necrosis.5
The main treatment for HSV encephalitis is IV acyclovir, which is associated with a significant decrease in morbidity and mortality, especially if started at the early disease course.2 Additional therapy with corticosteroids has shown improved outcomes in regard to the secondary effects of brain edema, but current guidelines remain controversial since there is the possibility that steroids could facilitate viral replication.2
— Paola Tabaro, MD, is a radiology resident at UConn Health at the University of Connecticut.
— Michelle Romero, MD, is an attending radiologist at Radiology Associates of Hartford in Connecticut.
— Alex Merkulov, MD, is an associate professor of radiology at UConn Health at the University of Connecticut.
References
1. Bradshaw MJ, Venkatesan A. Herpes simplex virus-1 encephalitis in adults: pathophysiology, diagnosis, and management. Neurotherapeutics. 2016;13(3):493-508.
2. Rabinstein AA. Herpes virus encephalitis in adults: current knowledge and old myths. Neuro Clin. 2017;35(4):695-705.
3. Hatanpaa KJ, Kim JH. Neuropathology of viral infections. Handb Clin Neurol. 2014;123:193-214.
4. Mahan M, Karl M, Gordon S. Neuroimaging of viral infections of the central nervous system. Handb Clin Neurol. 2014;123:149-173.
5. Steiner I, Benninger F. Manifestations of herpes virus infections in the nervous system. Neurol Clin. 2018;36(4):725-738.
