By Karen Stockman, CPC, PCS
Radiology Today
Vol. 11 No. 1 P. 10
The basic rules coders follow to choose the correct selective catheter code(s) can be mystifying. When you add distinctive vessel variations into the mix, further uncertainty ensues. When coders do not have a clear understanding of some common vessel variations—which can change code selection—choosing the correct code(s) can prove impossible.
There are two distinctive components to vascular interventional radiology (IR) coding: the imaging component and the surgical procedure component, the latter being the more complicated of the two. Catheter placements, which are considered a part of the surgical component, come in two flavors: selective and nonselective. Knowing when to code selective vs. nonselective is key to successful vascular IR coding. Nonselective catheter placement occurs when the catheter stays in the original vessel punctured or when it advances only to the aorta. Selective catheter placement occurs when a catheter advances from the original vessel punctured or from an artery that branches off the aorta.
Once the catheter reaches a vessel off the original vessel punctured or off the aorta, it becomes its own vascular family. This is important because coders must code to the highest level of selective catheter placement within a vascular family.


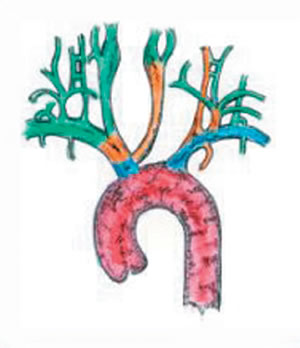
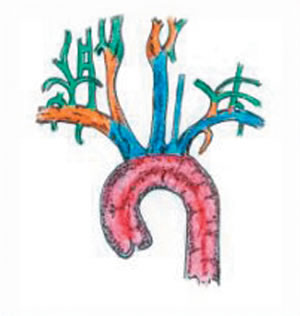
Three separate vascular families branch from the aortic arch. The images represent (from left to right) normal vessel anatomy of the vascular family: the right brachiocephalic, the left common carotid (LCC), and the left subclavian. When selecting vessels off the aortic arch, any of the three families entered must be coded to the highest level of selectivity. For example, if the right common carotid (RCC) artery, the LCC artery, and the left vertebral (LV) were selected, the following selective/surgical codes would be appropriate:
• RCC: 36216;
• LCC: 36215-59; and
• LV: 36216-59.
Another example of coding selective catheter placement for a patient with normal anatomy would be selective catheter placement of the right internal carotid artery (RT-ICA), the left internal carotid artery (LT-ICA), the left external carotid artery (LT-ECA), and the left thyrocervical artery (LT-TCA), making the following codes appropriate:
• RT-ICA: 36217;
• LT-ICA: 36216-59;
• LT-ECA: 36218 (each additional vessel selected in the same vascular family); and
• LT-TCA: 36216-59.
When a patient’s anatomy is unique or less common, choosing the correct selective catheter codes can become even trickier. Let’s take a closer look at some of the challenges coders encounter when coding variant anatomy. First, the definitions of the most common arterial variances are as follows:
• Common origin: A common origin variation is usually seen within the LCC artery and the right brachiochephalic arteries found in the cervicocerebral arch. Both arteries start with a wide-mouthed origin branching off the aorta. This type of vessel variance does not change selective catheter placement codes.

• Bovine arch: The bovine arch is found in the cervicocerebral arch and changes how the arteries branch off the aorta. The LCC artery branches off the right brachiocephalic trunk. In the coding world, this means the LCC, for selective purposes, is considered part of the right brachiocephalic family. Therefore, if selected, in addition to another artery off the right brachiocephalic family, the code for each additional vessel selected would be assigned.
• Separate origin: An artery that is normally found as part of another family has its own separate access off the aorta. This can be seen with the LV, which would make this a fourth family off the cervicocerebral trunk.
The following examples highlight instances where coders must grapple with variant anatomy rather than normal anatomy:
In the first example, a coder must code the same arteries selected for normal and common origin anatomy. Remember, the definition of a common origin is when arteries start with a wide-mouthed origin and both arteries arise off the aorta, which does not change the coding. Selected catheter placements in the RCC and the LCC arteries would be coded as follows:
| Arteries Selected | Normal Anatomy/CPT Code | Common Origin Anatomy/CPT Code |
| RCC | 36216 | 36216 |
| LCC | 36215-59 | 36215-59 |
For the second example, a coder must code the same arteries selected for normal anatomy and bovine origin anatomy. Remember, the definition of a bovine arch origin is an LCC artery coming off the right brachiochephalic trunk. Selected catheter placement of the RCC artery, the LCC artery, and the right vertebral (RV) would be coded as follows:
| Arteries Selected | Normal Anatomy/CPT Code | Common Origin Anatomy/CPT Code |
| RCC | 36218 | 36217 |
| LCC | 36215-59 | 36218 |
| RV | 36217 | 36218 |
Finally, in the third example, a coder would code the same arteries selected for normal anatomy and separate origin anatomy. Remember, the definition of separate origin is an artery that is normally found as part of another family that has its own separate access off the aorta. Selected catheter placement of the RCC artery, the LCC artery, and the LV would be coded as follows:
| Arteries Selected | Normal Anatomy/CPT Code | Common Origin Anatomy/CPT Code |
| RCC | 36216 | 36216 |
| LCC | 36215-59 | 36215-59 |
| LV | 36216-59 | 36215-59 |
— Karen Stockman, CPC, PCS, is the coding manager at CodeRyte.