By Kathryn Becker, MD, and Alex Merkulov, MD
Radiology Today
Vol. 21 No. 3 P. 30
History
A 32-year-old woman presented to the emergency department with acute right-sided flank pain associated with an urge to urinate. No chest pain, shortness of breath, headache, fever, leg swelling, or hematuria was reported. She stated that for the past two weeks she had been dealing with a cough and nasal congestion. CT of the abdomen and pelvis was performed to evaluate for nephrolithiasis. The imaging report from a prior chest CT performed at an outside institution, which was accessed through the EHR, noted dextrocardia.
Findings
The CT scout image demonstrated dextrocardia, the heart situated on the right side of the body with the cardiac apex pointing to the right (Figure 1). CT of the abdomen and pelvis, in axial and coronal planes, revealed a mirror-image transposition of the abdominal organs. The liver, gallbladder, and biliary system were located on the left side of the body. The spleen was abnormally located in the right upper abdominal quadrant. The stomach and descending colon were noted to be on the right side of the body, while the ascending colon was on the left side of the body. The abdominal aorta was positioned to the right of the inferior vena cava (Figures 2–5).
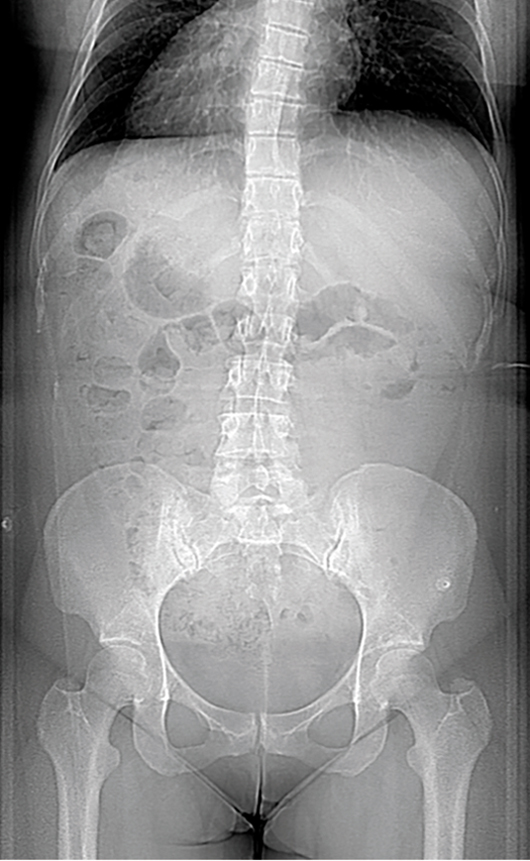
Figure 1
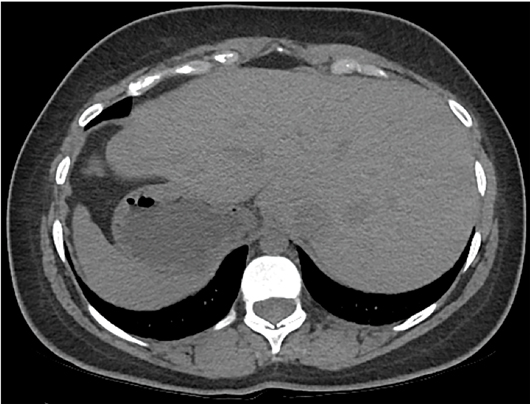
Figure 2
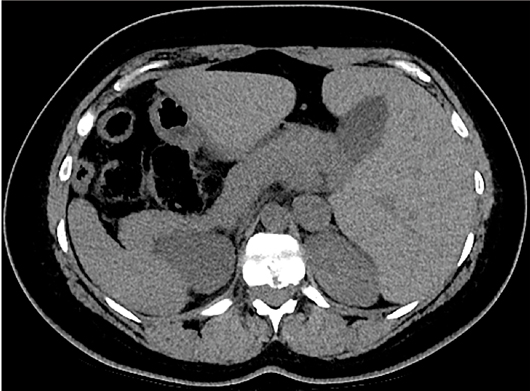
Figure 3
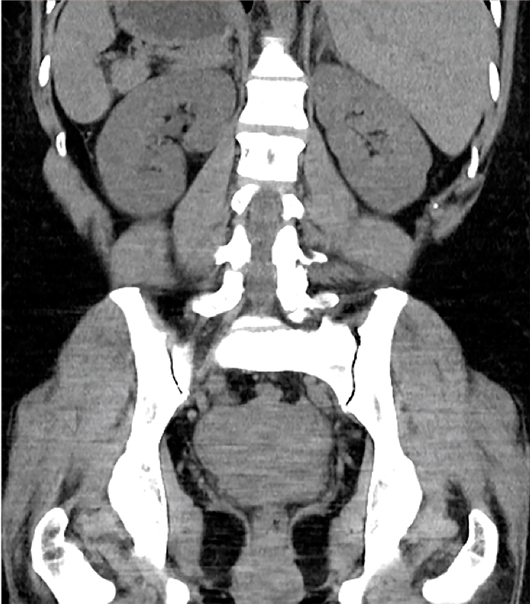
Figure 4

Figure 5
Diagnosis
Situs inversus totalis.
Discussion
Situs refers to the positioning of the heart and visceral structures in respect to the patient’s midline. Situs solitus refers to the normal, expected positioning of the heart and visceral structures, such that the cardiac apex, spleen, stomach, and aorta are to the left of the midline, while the liver and inferior vena cava are to the right of the midline.
In contrast to situs solitus, situs inversus is a term used to describe the inverted positioning of these structures. Situs inversus can be divided into situs inversus with dextrocardia (true mirror image), also known as situs inversus totalis, and situs inversus with levocardia. Situs inversus with dextrocardia is associated with only 3% to 5% incidence of congenital heart disease. Situs inversus with levocardia is much rarer, and affected individuals almost always have associated congenital heart disease. Situs inversus can be seen as a part of Kartagener syndrome, which is a subset of primary ciliary dyskinesia. Patients with Kartagener syndrome have situs inversus, chronic sinusitis or nasal polyposis, and bronchiectasis.
In contrast to both situs solitus and situs inversus, situs ambiguous refers to a disordered arrangement of the intrathoracic and intra-abdominal structures. Situs ambiguous is also known as heterotaxy syndrome. There is a high association of congenital heart disease in patients with heterotaxy syndrome, as well as malrotation of the bowel. Heterotaxy syndrome is often classified as heterotaxy with asplenia and heterotaxy with polysplenia.
Situs ambiguous with asplenia is also known as Ivemark’s syndrome or bilateral right sidedness. These patients demonstrate two right-sided lungs, meaning that both lungs have three lobes. They also have bilateral systemic atria with eparterial bronchus bilaterally (synonymous for the right superior lobar bronchus) and often have anomalous pulmonary venous return. As the name implies, the spleen is absent. This syndrome occurs more commonly in males, and patients have a poor prognosis; the majority of those affected die within the first year of life.
Situs ambiguous with polysplenia is also known as bilateral left sidedness. These patients demonstrate two left-sided lungs, meaning that both lungs have two lobes. They have bilateral pulmonary atria. As the name implies, these patients have multiple spleens. Patients with heterotaxy with polysplenia are more often female, and prognosis is more variable than is seen in heterotaxy with asplenia.
Situs inversus totalis can be diagnosed on radiography by evaluating the locations of the heart apex, aortic arch, and the stomach bubble and liver.
— Kathryn Becker, MD, is a radiology resident at UConn Health at the University of Connecticut.
— Alex Merkulov, MD, is an associate professor of radiology at UConn Health.
Resources
1. Fulcher AS, Turner MA. Abdominal manifestations of situs anomalies in adults. Radiographics. 2002;22(6):1439-1456.
2. Applegate KE, Goske MJ, Pierce G, Murphy D. Situs revisited: imaging of the heterotaxy syndrome. Radiographics. 1999;19(4):837-852; discussion 853-854.