Melody W. Mulaik, MSHS, CRA, FAHRA, RCC, RCC-IR, CPC, COC
Radiology Today
Vol. 21 No. 4 P. 26
Imaging pediatric patients can often take more effort and time than exams performed on adults. Additionally, physical considerations that come into play may change how the protocol of a study is defined. For these reasons, exams that are specifically defined for, or most commonly performed on, pediatric patients require extra attention.
Diagnostic Imaging
According to CPT Assistant, there are a few diagnostic imaging studies that are specifically defined for pediatric patients. The American Medical Association (AMA), the owner and publisher of the CPT procedure codes, defines an infant as a patient who is younger than 1 year old. There is a not a specific definition of a “child”; rather, the AMA states that the child code can be used for an exam of any patient who is small enough to fit on a single X-ray image. For code 76010, this would be less than 17 inches from nose to rectum.
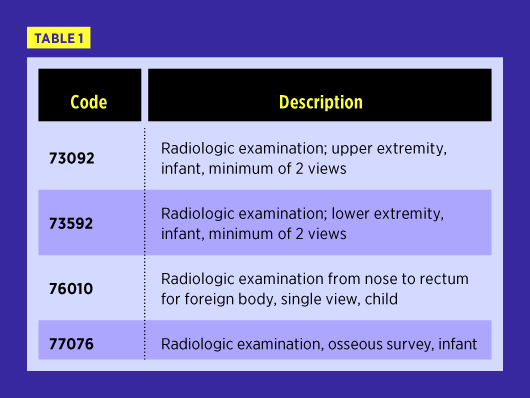
Procedure code 76010 is sometimes referred to as a “babygram” or “kiddiegram.” In some institutions, a babygram is defined as a single view chest and a single view abdomen of a neonate. In this situation, the radiologist should charge for interpretation of two exams, 71010 and 74000, even if both were taken on a single digital image or film, because interpreting neonatal chest and abdomen examinations is far more complex than interpreting a chest/abdomen view obtained for the express purpose of identifying a foreign body. The facility should charge for only one exam, however, since only one image was taken, according to the summer 2009 edition of Clinical Examples in Radiology.
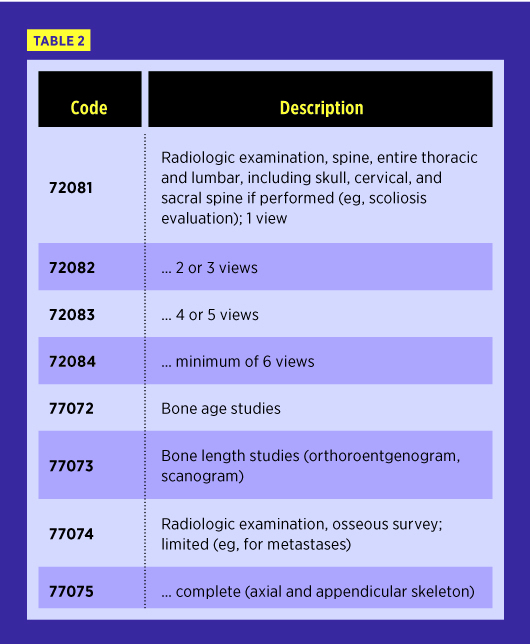
Other studies that are not specifically defined as pediatric but are most commonly performed on this patient population are scoliosis studies, bone age studies, bone length studies, and osseous surveys.
Ultrasound
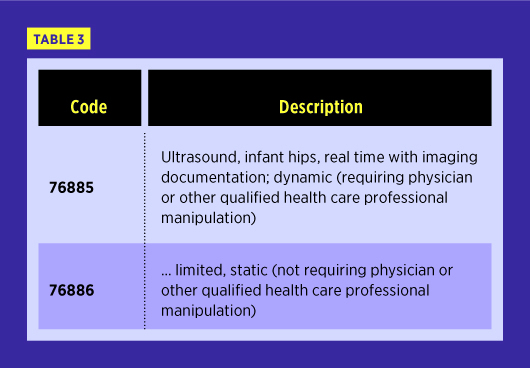
There are only two ultrasound codes that are specific to pediatric patients, and they address hip examinations on infants. It is important to note that in the CPT manual, the AMA includes the following definition of a qualified health care professional in the instructions for use of the CPT codebook: “A ‘physician or other qualified health care professional’ is an individual who is qualified by education, training, licensure/regulation (when applicable), and facility privileging (when applicable), who performs a professional service within his/her scope of practice and independently reports that professional service. These professionals are distinct from ‘clinical staff.’”
In addition to abdominal and retroperitoneal studies, other procedures that are frequently performed primarily on this patient population include intracranial and spinal canal studies.
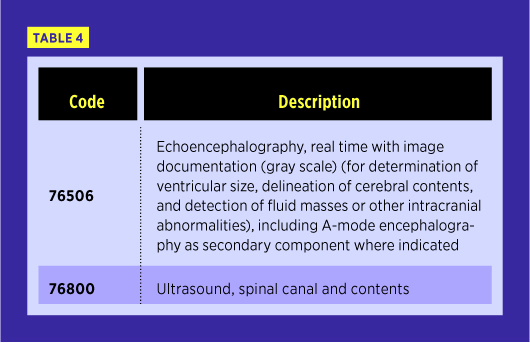
Procedure code 76506 defines an intracranial ultrasound exam that is often performed on infants with intracranial hemorrhage. It includes examination of the ventricles, brain substance, and intracranial vessels.
The spinal cord is visible on ultrasound exam in infants younger than 6 months old, but, after that time, it is hidden by the bones of the spine unless the patient has a posterior spinal defect. For this reason, ultrasound of the spinal canal is most often performed on infants. It can detect conditions such as tethered cord and spina bifida occulta.
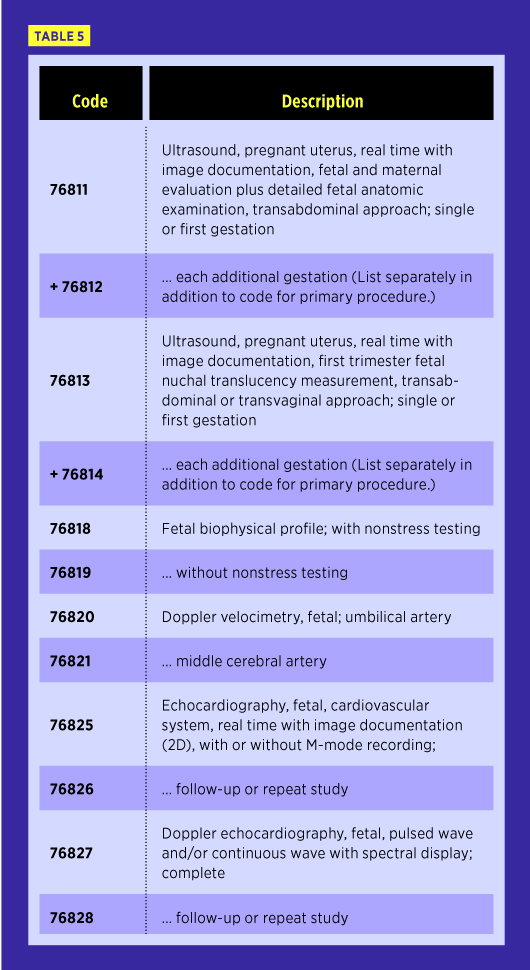
In addition to the regular obstetric ultrasound initial evaluation and follow-up codes, there are separate codes specifically for more detailed in utero fetal imaging of anatomic evaluation, fetal nuchal translucency, biophysical profile, Doppler imaging, and echocardiograms.
MRI
There are no pediatric-specific MRI codes and only two MRI codes that are specific to fetal imaging.
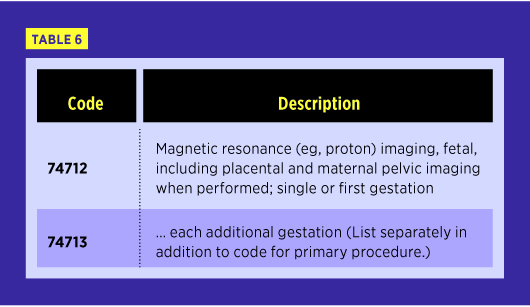
MRI can provide detailed anatomic information about an unborn child. In particular, fetal MRI is useful when ultrasound suggests an abnormality but does not provide a definitive answer.
Other Modalities
There are no pediatric-specific codes for CT or nuclear medicine—including PET.
Summary
While the vast majority of procedure codes are not defined by a patient’s age, it is important to be aware of the few that are, in order to maintain appropriate coding and billing practices. The work involved with pediatrics can be time consuming, and organizations want to ensure that they are reporting these procedures correctly.
— Melody W. Mulaik, MSHS, CRA, FAHRA, RCC, RCC-IR, CPC, COC, is the president of Coding Strategies, Inc, and Revenue Cycle, Inc.