By Pramod Gupta, MD, and Soume Foshee, MD
Radiology Today
Vol. 20 No. 5 P. 30
History
A 65-year-old man with history of cirrhosis underwent CT imaging of the abdomen and pelvis for an evaluation of nonspecific abdominal pain. On CT imaging, a solid mass was identified in his right lateral breast. He was subsequently referred for diagnostic mammography and a targeted ultrasound to further characterize the right breast mass.
Findings
Axial CT image demonstrates bilateral gynecomastia and an isodense to the gynecomastia solid mass in the right lateral breast (Figure 1). Right breast spot compression mediolateral oblique and full-field craniocaudal mammographic views demonstrate a round equal density mass with irregular margins (Figures 2 and 3), which correlates with the mass noted on CT. Targeted ultrasound of the right breast at 9:00 at middle depth revealed an irregular, suspicious for malignancy mass with marked associated posterior shadowing (Figure 4). An ultrasound-guided biopsy was performed, and the patient subsequently underwent a surgical excision of the mass.
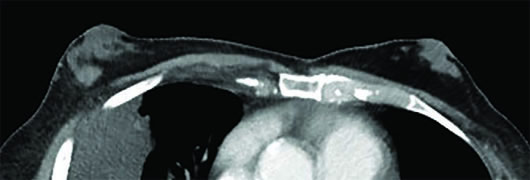
Figure 1
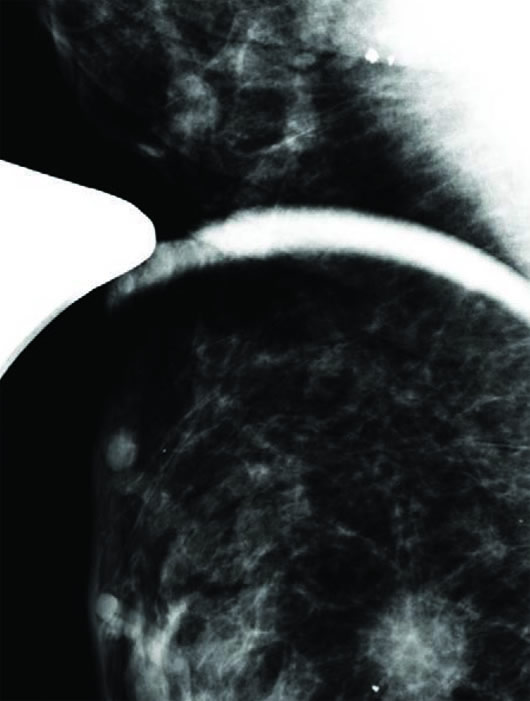
Figure 2
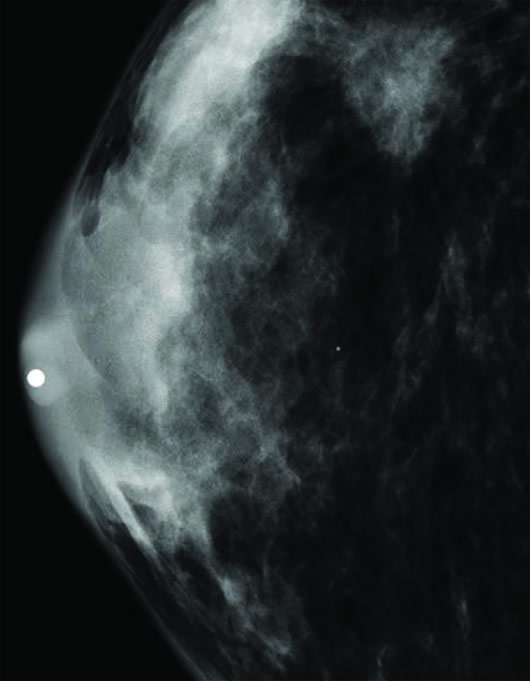
Figure 3
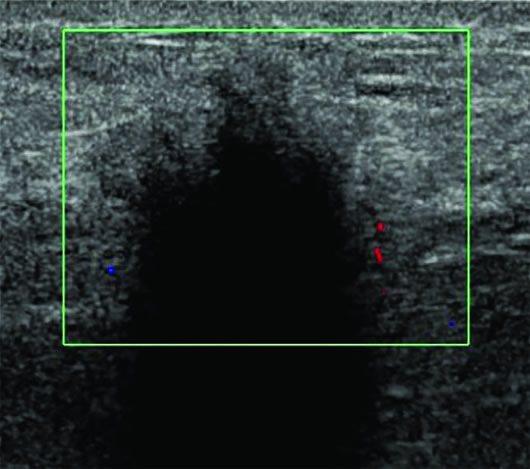
Figure 4
Diagnosis
Granular cell tumor (GCT) of the breast.
Discussion
GCT is a soft tissue neoplasm that originates in the nervous system and is mainly found in the skin, oral cavity, or digestive tract. Only 5% to 8% of GCTs are found in the breast, with a male-to-female ratio of 1:9. These tumors most commonly occur in women between 30 and 50 years of age, with a frequency of approximately 1 in 1,000 breast cancers. GCT of the breast arises from intralobular breast stroma and occurs within the distribution of the cutaneous branches of the supraclavicular nerve. The most widely accepted theory is that GCT is of a Schwann cell origin.
Clinically, GCT presents as a painless firm breast mass, which can be fixed to the skin or chest wall. Clinically and on imaging, GCT is often indistinguishable from breast cancer.
On mammography, the tumor presents as a mass lesion with an irregular margin. On ultrasound, GCT can have a variable appearance with varying echogenicity, poorly defined margins, and posterior shadowing. Conversely, it may appear as a hypoechoic, circumscribed mass with posterior enhancement, mimicking the appearance of a cyst. Positive immunohistochemical staining of the cells for S-100, neuron-specific enolase, and carcinoembryonic antigen proteins are indicative of GCT.
Surgery is the mainstay of treatment for GCT, and there is no role for adjuvant therapy. Resection with adequate margins is necessary because the tumor has no capsule. Rarely (<2%), the GCT is malignant. Metastasis to liver, lung, bone, and axillary lymph nodes are reported with malignant GCT.
— Pramod Gupta, MD, is a staff radiologist at the Dallas VA Medical Center.
— Soume Foshee, MD, is a staff radiologist at the Dallas VA Medical Center.
Resources
1. Patel HB, Leibman AJ. Granular cell tumor in a male breast: mammographic, sonographic, and pathologic features. J Clin Ultrasound. 2013;41(2):119-121.
2. Adeniran A, Al-Ahmadie H, Mahoney MC, Robinson-Smith TM. Granular cell tumor of the breast: a series of 17 cases and review of the literature. Breast J. 2004;10(6):528-531.
3. Doğan L, Atalay C. Benign mesenchymal breast tumors. J Breast Health. 2011;7(3):149-153.