
On the Case
By Pramod Gupta, MD, and Soume Foshee, MD
Radiology Today
Vol. 19 No. 6 P. 28
History
A 61-year-old woman presented with a palpable right breast mass that had been present for two months. Right breast mammography was obtained, followed by a targeted right breast ultrasound. Her previous mammogram, performed two years prior at an outside institution, was not available for comparison. According to the patient, prior mammography results were reported to her as benign. The only other relevant past medical history included COPD and hyperlipidemia.
Findings
Right breast craniocaudal and mediolateral oblique full-field mammographic images with a palpable triangular skin marker in place demonstrate a high-density anterior depth mass centered between 10:00 and 12:00 (Figures 1 and 2). Vascular calcifications are also noted above the nipple line at anterior depth. Targeted right breast ultrasound demonstrates a morphologically suspicious, heterogeneous, nonshadowing, hypoechoic mass with a peripheral hyperechoic rim (Figures 3 and 4). This palpable mass was centered at 11:00 at anterior depth. An ultrasound-guided biopsy was recommended and performed. Subsequently, the patient underwent a surgical excision of this mass.
Figure 1 |
Figure 2 |
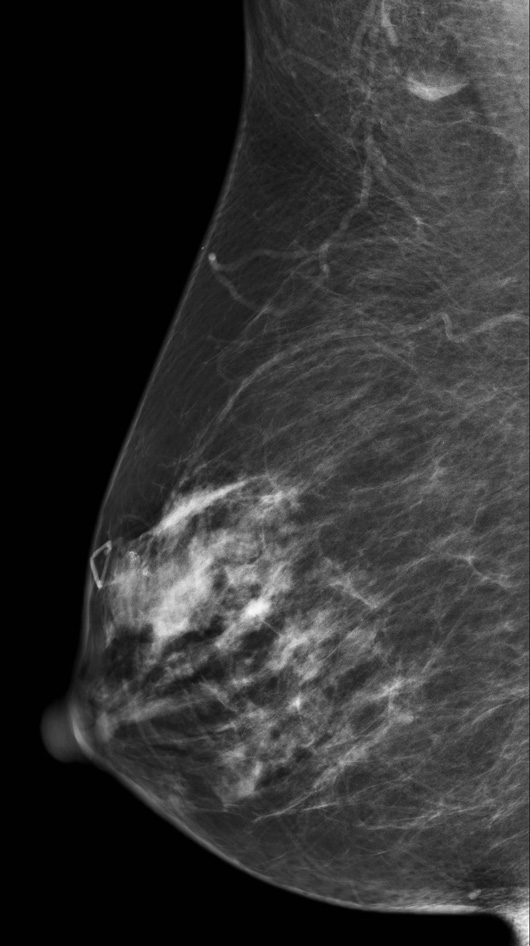
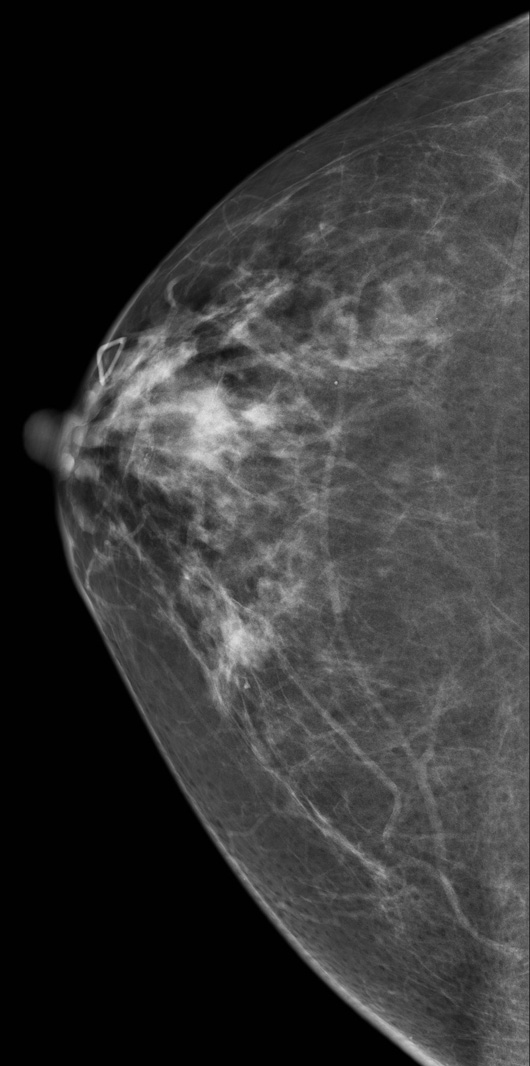
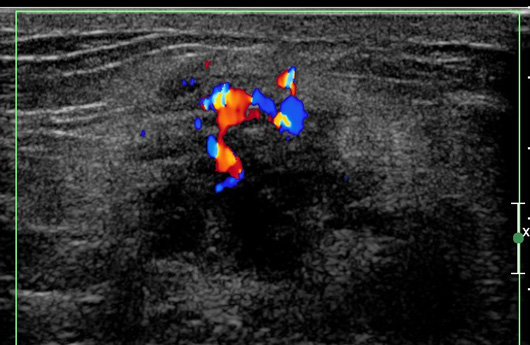
Figure 3
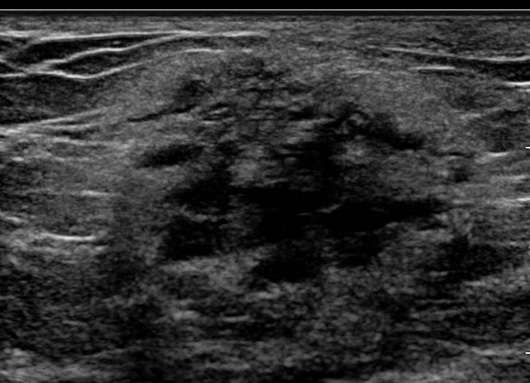
Figure 4
Diagnosis
Lymphocytic mastitis.
Discussion
Lymphocytic mastitis, or diabetic mastopathy, is an unusual finding in patients with early-onset and longstanding diabetes. It can present as a nontender or tender palpable breast mass. Mammography and ultrasound frequently demonstrate findings suspicious for malignancy, thus biopsy and histological confirmation is usually required.
Lymphocytic mastitis can also mimic breast cancer on physical examination. Multicentric or bilateral involvement has been reported. Masses also may appear in a wide range of sizes. They can be palpable or only detected radiologically. They can occur in any breast quadrant, although they do have a propensity to develop in the retro-areolar region.
Mammography has not generally been sensitive in characterizing these masses. Ultrasound is the most useful adjunctive tool to mammography in evaluating a palpable mass in a patient suspected of having diabetic mastopathy. On ultrasound, these masses are usually irregular, hypoechoic, and can be associated with acoustic shadowing.
Differential diagnoses for lymphocytic mastitis or diabetic mastopathy include granulomatous mastitis, fibrotic tissue, and breast carcinoma. In view of suspicious clinical and radiological findings, tissue diagnosis is typically mandatory in these cases.
Ultrasound-guided core needle biopsy is a reliable method for establishing a tissue diagnosis and can eliminate the need for more aggressive procedures, such as a surgical biopsy. Lymphocytic mastitis is a benign mass, and there is no evidence to support development of breast cancer from diabetic mastopathy. In patients with diabetes, the recurrence rate for lymphocytic mastitis can be as high as 32%.
— Pramod Gupta, MD, is a staff radiologist at the Dallas VA Medical Center.
— Soume Foshee, MD, is a staff radiologist at the Dallas VA Medical Center.
Resources
1. Schwartz IS, Strauchen JA. Lymphocytic mastopathy: an autoimmune disease of the breast? Am J Clin Pathol. 1990;93(6):725-730.
2. Sabaté JM, Clotet M, Gómez A, De Las Heras P, Torrubia S, Salinas T. Radiologic evaluation of uncommon inflammatory and reactive breast disorders. Radiographics. 2005;25(2):411-424.
3. Ghosh S, Collier A, Simpson C, Malik I, Milne A. Diabetic mastopathy. Pract Diabetes Int. 2008;25(1):10-11.
4. Sotome K, Ohnishi T, Miyoshi R, et al. An uncommon case of diabetic mastopathy in type II non-insulin dependent diabetes mellitus. Breast Cancer. 2006;13(2):205-209.