By Alex Merkulov, MD
Radiology Today
Vol. 20 No. 8 P. 30
History
A 58-year-old man presented to the gastrointestinal clinic for a consultation of his dysphasia. The patient reported solid food dysphagia for the past 12 months, and his symptoms were getting progressively worse. He had previously undergone a modified barium swallow and a speech evaluation, which were both normal. The patient was found to have elevated integrated relaxation pressure on a high-resolution esophageal motility study with intact peristalsis, which excluded achalasia, and was consistent with esophagogastric junction outflow obstruction. Chest CT with IV contrast was ordered to evaluate the gastroesophageal junction and to exclude malignancy. The patient was also scheduled for an endoscopy and placed on a soft diet.
Findings
Axial, coronal, and sagittal IV contrast-enhanced (60 mL of Omnipaque-350) CT images of the chest demonstrated a 3.5-cm smoothly marginated, homogeneous, soft tissue distal esophageal mass located just above the gastroesophageal junction (Figures 1, 2, 3, and 4). The mass lacked cystic or calcified components. There was no mediastinal or hilar lymphadenopathy. The patient underwent an endoscopic ultrasound (EUS) with a fine needle aspiration for a tissue diagnosis of the distal esophageal mass.
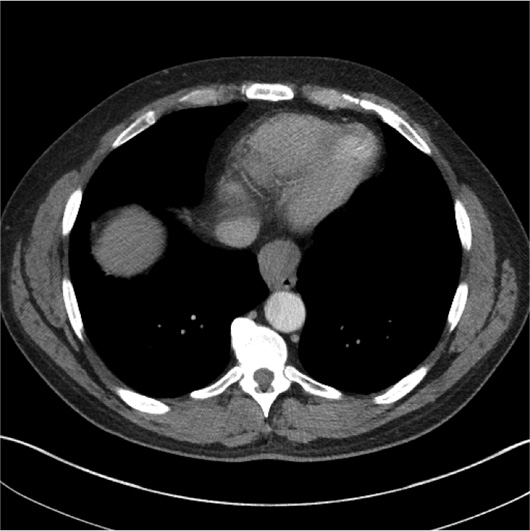
Figure 1
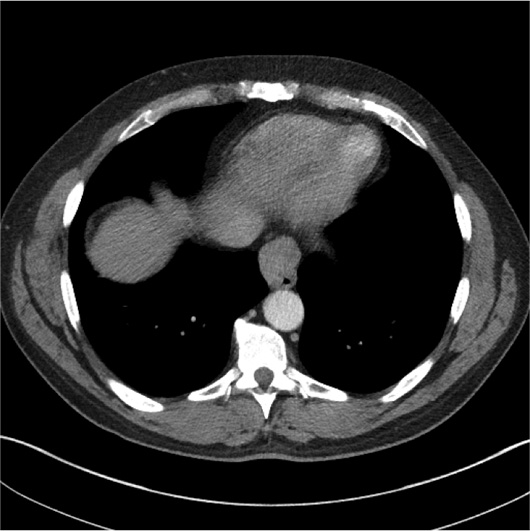
Figure 2
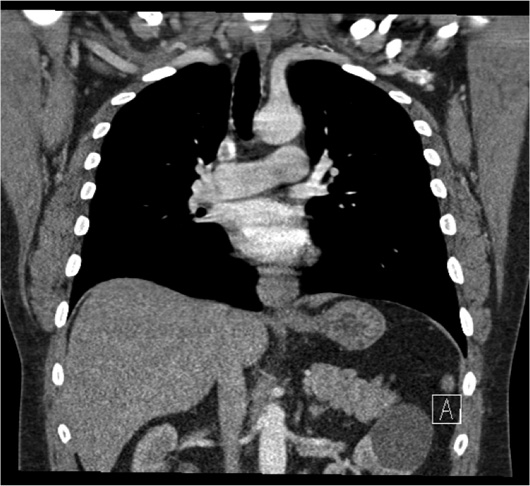
Figure 3

Figure 4
Diagnosis
Esophageal leiomyoma.
Discussion
Benign esophageal tumors represent 20% of esophageal neoplasms. Imaging findings of benign tumors include a smooth intramural or intraluminal mass without ulceration or nodularity and absence of peritumoral invasion, lymphadenopathy, or distant metastases.
Leiomyomas are neoplasms of mature smooth muscle cells and are the most common benign esophageal neoplasm, although they are about 50 times less common than esophageal carcinoma. Leiomyomas are usually less than 3 cm in size and are found predominantly in the middle and lower thirds of the esophagus, the portion of the esophagus lined by smooth muscle.
Leiomyomas appear smooth or slightly lobulated and may contain course calcification, but cystic degeneration, necrosis, and ulceration almost never occur. Approximately 97% of leiomyomas are intramural, with 10% of these masses having a circumferential growth pattern.
On barium examination, leiomyomas exhibit the typical findings of an intramural mass, appearing as smooth-surfaced crescent-shaped filling defects that form right angles or slightly obtuse angles with the adjacent esophageal wall. They can occasionally encircle the esophagus, producing a short stricture.
On CT, esophageal leiomyomas are smoothly marginated homogeneous masses in the mid to lower esophagus, occasionally containing areas of calcification. These tumors are isoattenuating or hypoattenuating to muscle on nonenhanced CT and slightly hyperintense on T2-weighted MR imaging. They demonstrate homogeneous enhancement after contrast administration.
EUS can facilitate diagnosis and guide the treatment approach by demonstrating which layer of the esophageal wall is involved. EUS findings of a homogeneous hypoechoic mass in the muscularis mucosae, submucosa, or muscularis propria with an intact overlying mucosa have a diagnostic accuracy of 89% for esophageal leiomyoma. FDG PET exams are usually negative in patients with leiomyomas, as these tumors have a low mitotic rate, although FDG uptake has occasionally been reported.
The differential diagnosis for intramural masses in the esophagus includes duplication cysts, granular cell tumors, gastrointestinal stromal tumors (GISTs), lymphoma, and hematogenous metastases. Duplication cysts are the second most common benign esophageal lesions after leiomyomas but usually manifest in childhood and have typical findings of cysts with all imaging modalities. Granular cell tumors of the esophagus may be indistinguishable from leiomyomas but are much less common and tend to be multiple.
Calcification has been reported to be a specific finding of leiomyomas but can also occur in esophageal GISTs. Large GISTs may be differentiated by central low attenuation secondary to necrosis or cyst formation. Small GISTs may be homogeneous intramural masses indistinguishable from leiomyomas. Immunohistochemical analysis helps distinguish esophageal leiomyomas from GISTs, as the former are negative for CD117 and CD34.
Most patients with an esophageal leiomyoma are asymptomatic, but dysphagia and pain may develop, depending on the size of the lesion and amount of encroachment on the esophageal lumen. Unlike patients with malignant esophageal tumors, affected individuals usually have longstanding symptoms, with a duration of more than two years in most cases.
Treatment options include endoscopic resection, surgical enucleation, and observation. Esophageal leiomyomas have a benign clinical course and typically do not recur after surgery.
— Alex Merkulov, MD, is an associate professor of radiology at UCONN Health.
Resources
1. Levine MS. Benign tumors of the esophagus. In: Gore RM, Levine MS, eds. Textbook of Gastrointestinal Radiology. 3rd ed. Philadelphia, PA: Saunders; 2008:401-416.
2. Xu GQ, Qian JJ, Chen MH, Ren GP, Chen HT. Endoscopic ultrasonography for the diagnosis and selecting treatment of esophageal leiomyoma. J Gastroenterol Hepatol. 2012;27(3):521-525.
3. Mutrie CJ, Donahue DM, Wain JC, et al. Esophageal leiomyoma: a 40-year experience. Ann Thorac Surg. 2005;79(4):1122-1125.