By Mark Koeniguer
Radiology Today
Vol. 20 No. 9 P. 8
The FDA recently announced draft regulations that would mandate density notification for all women undergoing mammography screening. Assuming the FDA regulations move forward, how might they shift screening toward a more personalized approach and significantly improve cancer detection for women at higher risk?
At the same time, controversy swirls around the recommended screening age and frequency. Several medical and advocacy organizations have published screening guidelines intended for women at average risk of developing breast cancer. Risk, however, is calculated based on multiple factors, such as gynecological and family history, age, and genetics, plus one of the strongest risk factors: breast density.
According to a study by Kerlikowske in the New England Journal of Medicine, women with dense breasts have up to a 17-fold increase of being diagnosed with an interval breast cancer when compared with women with less dense breasts. In addition, these interval cancers are twice as likely to be invasive and almost four times as likely to be classified as an advanced-stage cancer, according to a study by Puliti and colleagues in Breast Cancer Research.
Breast Density and Triage
Given the associated risks, breast density becomes a critical component in triaging women to appropriate screening. While mammography remains the gold standard for screening, these risks indicate that, for women with dense breasts, something more must be done.
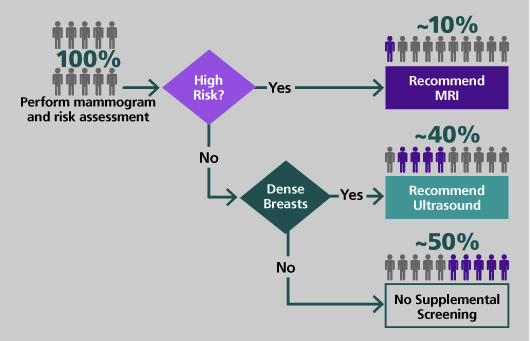
A triage plan based on breast density can be quite straightforward. For instance, the breast care team employs a breast cancer risk model that considers family history, gynecological history, and breast density to identify those women at high risk of developing breast cancer. Of the remaining women, those with high breast density are at greater risk of interval cancer due to masking. Radiologists and referring physicians can work together to create, for women in each of these groups, personalized screening plans that increase the likelihood of early detection. Many breast care teams use this approach to offer supplemental screening—a functional imaging modality such as breast MRI (or perhaps contrast-enhanced mammography, if MRI is contraindicated) for women at high risk, or ultrasound for women with dense breast tissue at low or average risk of developing breast cancer.
Improved Assessment
Evaluating the two aforementioned risks requires breast density assessment with the reliability of a medical test. Traditionally, radiologists have visually assessed breast density for inclusion in the mammography report, but such assessments have been shown to suffer significant inter- and intrareader variability as well as imaging equipment variability due to image processing and imaging modes used. New technology, validated for both risk assessment and identification of dense breasts, means that an objective, repeatable, and automated test can now replace visual assessment. Advantageously, as is suggested in the 5th Edition of BI-RADS, automated software provides volumetric breast density assessment reflecting the proportion of dense tissue that would be found on breast MRI.
Automated breast density software solves the fundamental problems of providing a reliable density measure for risk assessment and triage. A woman’s breast density will no longer subjectively differ from exam to exam or depend on which radiologist reads her mammogram, thus affecting the personalized breast screening plan she is offered. The software also provides a defensible assessment that ensures proper justification for the costs associated with supplemental screening and can be used to help garner reimbursement for supplement screening.
To date, according to a 2019 article by Brentnall and colleagues in the Journal of Breast Imaging, one automated volumetric breast density software, VolparaDensity, has now been included and validated in the Tyrer-Cuzick v8 (TC8) breast cancer risk model.
The Next Step
Joseph P. Russo, MD, section chief of women’s imaging at St. Luke’s University Health Network and a clinical assistant professor at Philadelphia’s Temple University School of Medicine, describes how personalized screening builds on traditional mammography and breast density notification.
“Breast density notification standardization across the United States is an acknowledgment of the fact that breast imaging has become more complicated since the incredible success of mammography,” Russo says. “We are now obligated to take the next step toward a personalized approach to breast imaging based on patient risk and breast density.
“Adjuncts to traditional screening mammography significantly aid in the early detection of breast cancer, specifically in dense breast patients,” Russo continues. “Radiologists have become experts in detecting even the smallest signs of breast cancer on mammograms, an expertise that is often rendered useless in dense breast patients. New screening modalities allow clinically significant cancers to be discovered that were potentially undetectable with mammography. This could translate into the next leap in breast cancer survival, like the one experienced with mainstream mammography screening.”
Personalized Screening Plans
Implementing a personalized screening program based on breast cancer risk and breast density should include the following steps:
• Technology implementation. Work with your IT team to automate volumetric breast density insertion into TC8.
• Triage design. Decide the clinical thresholds for lifetime risks and for determining whether a woman has dense breasts.
• Workflow deployment. Train technologists and radiologists on the triage design and patient workflow. Work with staff on gaining referring physician scripts for supplemental screening.
• Outreach. Educate referring physicians about personalized screening and how it benefits their patients. Provide women with dense breasts or a high lifetime risk of developing breast cancer additional information about their screening options.
New Protocols in Action
Eric J. Kraemer, MD, radiologist at Reno Diagnostic Centers, has incorporated such a screening protocol in his practice.
“Incorporating an objective density measure and the Tyrer-Cuzick risk model has allowed us to better personalize screening for all of our patients,” Kraemer says. “Patients with a lifetime risk of greater than 20% are recommended for mammography and MRI screening. The personalized plan for patients with dense breasts but with lower risk includes mammography and automated breast ultrasound. For patients who do not have dense breasts and are at low risk of developing breast cancer, mammography continues to be the gold standard in breast cancer screening. Developing a personalized breast care for each woman depending on her specific risk factors means that we can do a better job at detecting cancer earlier, ensuring that lives are saved.”
Moving beyond breast density notification, radiologists and primary care physicians must now work together to make sure that a personalized breast care program follows best practices. Only then will they be able to ensure that every woman receives a screening protocol guided by her personal risk factors.
— Mark Koeniguer is the president and chief commercial officer of Volpara Solutions.