 On the Case
On the Case
By Jasmeet Singh, MD; Anna Luisa Kuhn, MD, PhD; and Ajit S. Puri, MD
Radiology Today
Vol. 23 No. 5 P. 30
History
A 35-year-old man presented to the emergency department with altered mental status and on workup was found to be positive for COVID-19 (unvaccinated). CT imaging of the brain was performed.
Findings
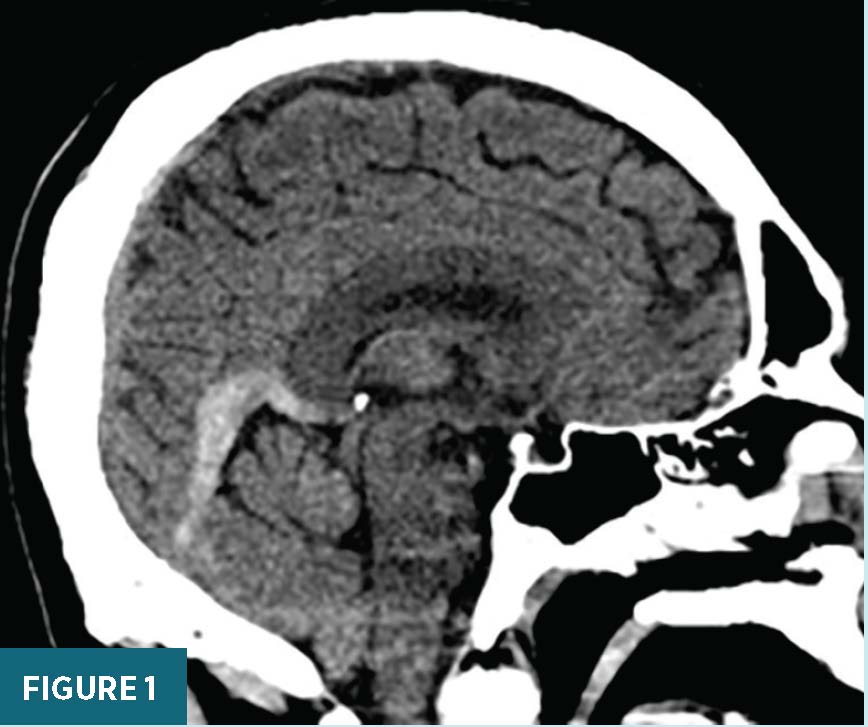
Noncontrast sagittal head CT image showed hyperdense material in the vein of Galen, straight sinus, and torcula, consistent with clot (Figure 1).
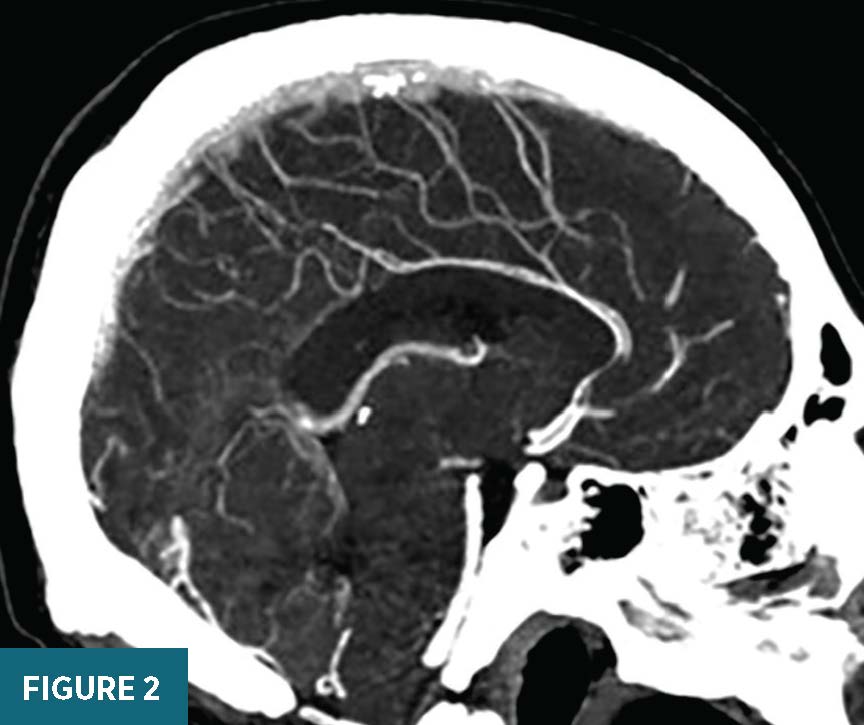
Sagittal CT angiogram image of the head revealed no flow in the vein of Galen, straight sinus, and torcula, consistent with occlusion (Figure 2).
Lateral view angiogram of the head showed no filling of the vein of Galen, straight sinus, and torcula. Cortical veins, superior sagittal sinus, and transverse and sigmoid sinuses are patent (Figure 3).
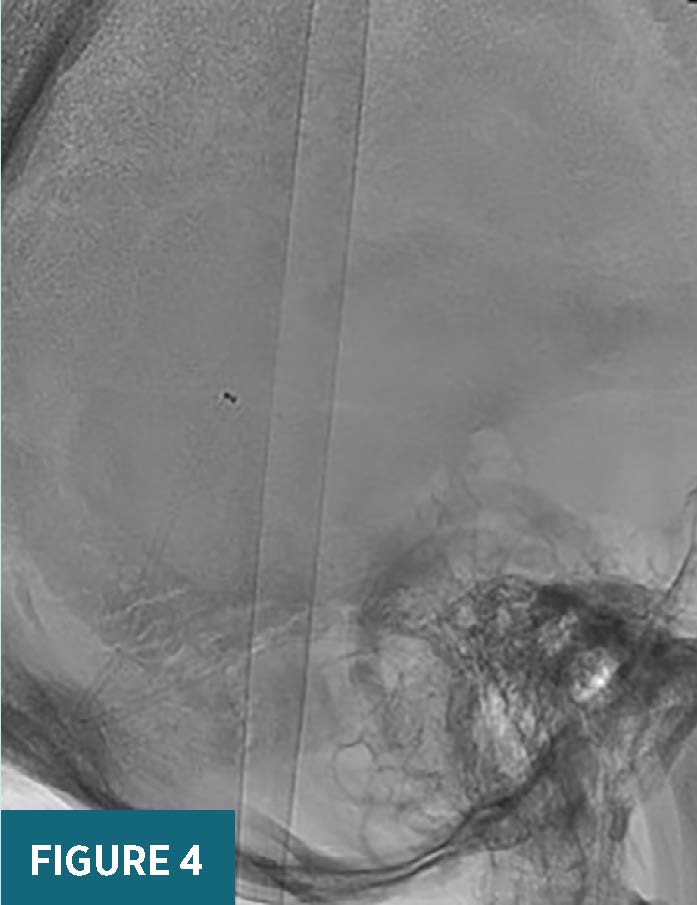
Lateral intraprocedural radiograph of the head showed an aspiration catheter in the straight sinus (Figure 4).
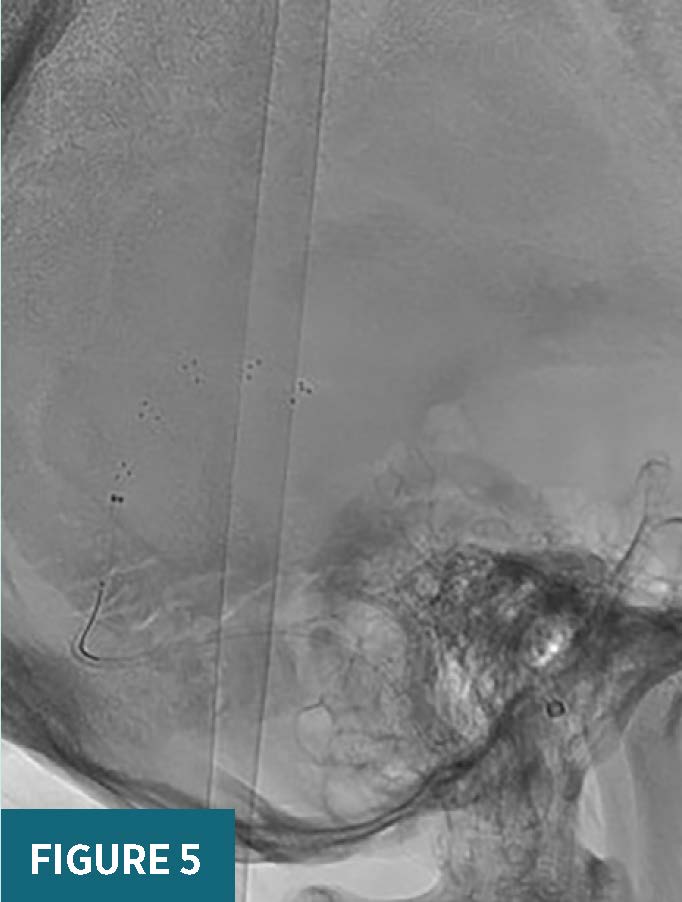
Lateral intraprocedural radiograph of the head showed a stent-retriever spanning from the vein of Galen into the straight sinus (Figure 5).
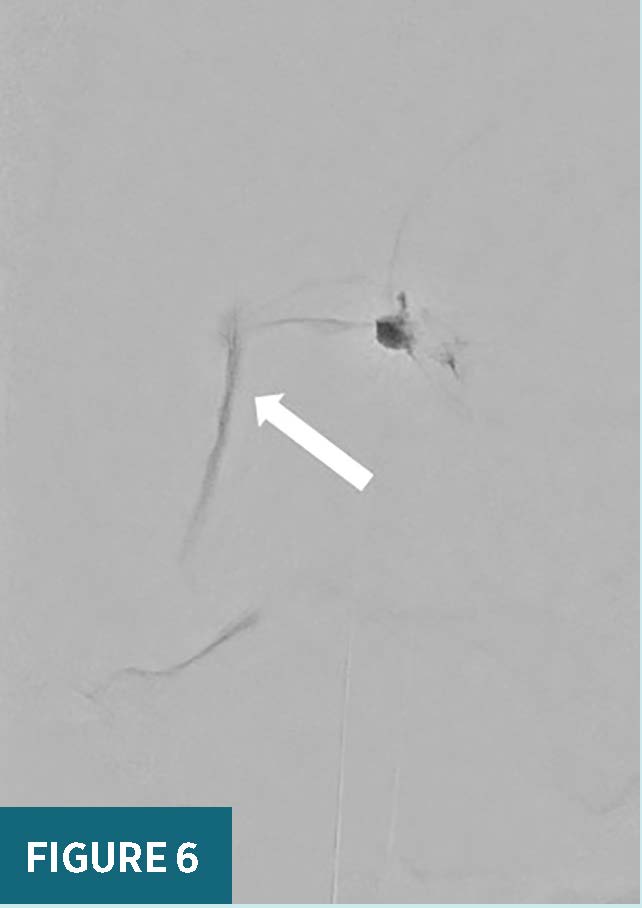
Follow-up lateral view angiograms after the thrombectomy passes demonstrated delayed appearance of a small channel of flow (arrow) through the vein of Galen into the straight sinus and torcula (Figure 6).
Follow-up sagittal CT angiogram image of the head one day after the procedure showed restoration of flow through the deep venous system with small areas of nonflow limiting residual clot along the straight sinus (Figure 7).


Diagnosis
Cerebral venous sinus thrombosis (CVST).
Discussion
CVST is a rare cause of stroke and is associated with high risk of morbidity and mortality, if not recognized and treated early. CVST accounts for approximately 0.5% to 1% of stroke admissions and is more common in females than males.1 Risk factors for CVST include sickle cell anemia, thalassemia, dehydration, iron deficiency, pregnancy, puerperal period, oral contraceptive pill use, cancer, intracranial hypertension, Crohn’s disease or ulcerative colitis, and collagen vascular diseases (Lupus, Wegner’s granulomatosis, or Behcet syndrome).
A hypercoagulable state is a well-known risk factor for CVST, and patients with COVID-19 are known to develop thrombotic complications, such as pulmonary embolism, venous thromboembolism, and sinus venous thrombosis.2-4
CVST can present with nonspecific symptoms, such as headache, seizures, and altered mental status. Strokelike neurological symptoms are seen in up to 40% of patients, with motor deficits being the most common, followed by visual impairment and aphasia. The diagnosis is usually made on a CT angiogram or CT venogram of the head, which will show the absence of flow in the affected sinus(es). Prompt diagnosis and treatment are important for patient recovery.
Generally, CVST has a favorable prognosis with complete functional recovery in about 75% of patients.1 Factors associated with poor outcome include male sex, confusion or coma as a presenting symptom, intracranial hemorrhage, deep venous system involvement, concomitant infection, or malignancy.1
First line treatment of CVST consists of anticoagulation therapy with heparin. However, patients who do not improve, who continue to deteriorate on anticoagulation therapy, or in whom the deep venous system (intracerebral veins, basal veins of Rosenthal, vein of Galen, straight sinus) is involved can be considered for endovascular therapy.
Anticoagulation prevents the progression of a thrombus in the venous system and affects the balance between thrombosis and lysis. Endovascular treatment aims to reduce the existing thrombus burden and restore flow in the affected sinus(es). Endovascular therapy may consist of clot aspiration, stent-retriever thrombectomy, or a combination of the two. Additionally, thrombolytic agents can be directly infused at the site of the clot.5
As in our case, restoration of a small channel of flow can be sufficient to reestablish venous drainage and help increase the effect of anticoagulation. The patient was maintained on a high intensity heparin drip with an activated partial thromboplastin time goal of 55 to 75 postprocedure. The patient improved neurologically with only some headache remaining. After discharge, the patient will continue oral anticoagulation medication (Eliquis or Xarelto) for six months.
The recurrence risk of CVST is about 2% to 7%.6 Unfortunately, despite good physical recovery, some patients experience symptoms of anxiety, depression, or cognitive impairment.7
— Jasmeet Singh, MD, is an associate professor in the division of neurointerventional radiology in the department of radiology at the University of Massachusetts Medical Center in Worcester.
— Anna Luisa Kuhn, MD, PhD, is an assistant professor in the division of neurointerventional radiology in the department of radiology at the University of Massachusetts Medical Center.
— Ajit S. Puri, MD, is a professor in the division of neurointerventional radiology in the department of radiology at the University of Massachusetts Medical Center.
References
1. Ulivi L, Squitieri M, Cohen H, Cowley P, Werring DJ. Cerebral venous thrombosis: a practical guide. Pract Neurol. 2020;20(5):356-367.
2. Klok FA, Kruip MJHA, van der Meer NJM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020;191:145-147.
