By Fatima Khan, BS; Daniel Chen, MD; and Marco Molina, MD
Radiology Today
Vol. 21 No. 7 P. 30
History
A 67-year-old man with a past medical history of benign prostatic hypertrophy presented to the emergency department with acute onset of unilateral testicular pain associated with nausea, vomiting, and difficulty urinating. He denied fevers, chills, abdominal pain, and dysuria. Prior to presentation, the patient was seen at an urgent care center and diagnosed with urinary retention, for which a straight catheter was inserted. However, catheterization revealed no urine in his bladder. The patient’s vitals on presentation were unremarkable. Physical exam revealed only tenderness to palpation in the abdominal right lower quadrant. Complete blood count and basic metabolic panel revealed leukocytosis measuring 12 X 109 cells/L. Urinalysis revealed trace leukocytes and red blood cells measuring >50 per high power field. An ultrasound of the testes and CT of the abdomen and pelvis were ordered to rule out referred pain from a kidney stone or appendicitis.
Findings
Axial, sagittal, and coronal contrast-enhanced CT images of the abdomen and pelvis revealed a 5 mm ureterolith at the right ureterovesicular junction (not shown), with mild right hydroureteronephrosis (Figures 1 and 2). The right and left kidneys were fused to the left of the abdominal midline, with separate collecting systems and ureters (Figures 3, 4, and 5). The left renal moiety cortex, hila, and collecting system were oriented normally without hydroureteronephrosis (Figure 6). The crossed, fused right renal moiety was oriented craniocaudally and medially in the coronal plane in reference to the left moiety (Figure 4). Moreover, the crossed right renal moiety is malrotated with an inferolaterally oriented hilum, consistent with sigmoid configuration (Figure 4).
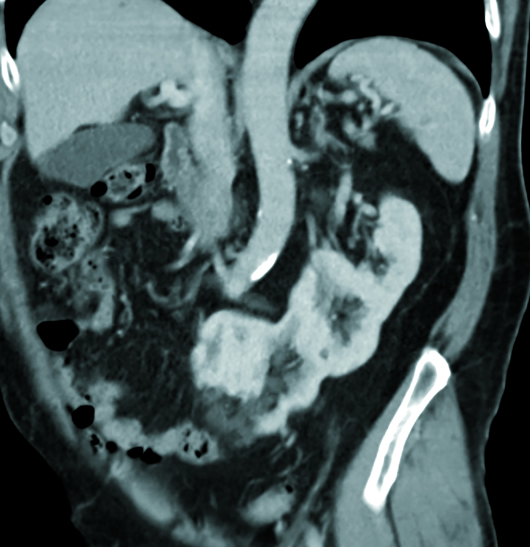
Figure 1

Figure 2
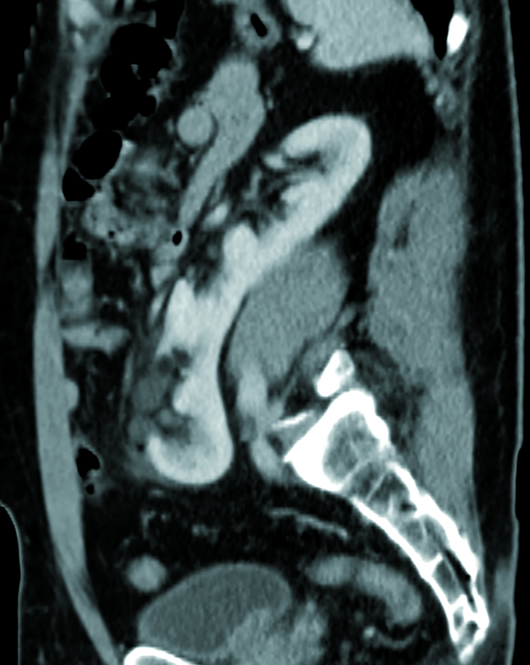
Figure 3
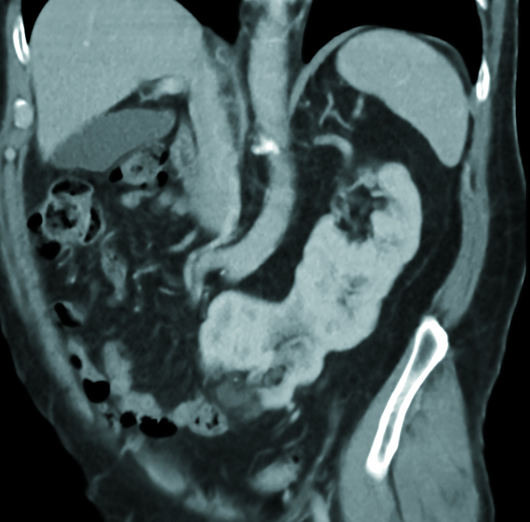
Figure 4
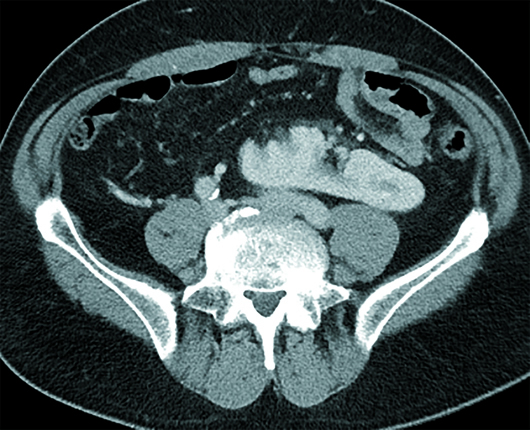
Figure 5

Figure 6
Diagnosis
Crossed-fused renal ectopia (CFRE).
Discussion
CFRE is a rare congenital anomaly in which a kidney crosses the midline and becomes fused with the opposite kidney. The ureter of the ectopic kidney re-crosses at the midline to insert at the ureteropelvic junction on the opposite, but anatomically correct, side. Most cases of CFRE are asymptomatic and typically diagnosed incidentally on imaging. A subset of cases is symptomatic and may present with flank pain, a palpable renal mass, dysuria, frequency, and urgency.
Renal ectopia refers to congenital renal anomalies in which a kidney is in abnormal position due to aberrant ascent during development. In simple renal ectopia, the kidney is on the correct anatomical side. In crossed renal ectopia (CRE), an ectopic kidney crosses the midline and lies on the side opposite to its ureteral attachment to the bladder. The crossed kidney may be fused or unfused to the adjacent kidney. The estimated incidence of CRE ranges from 1:2,000 to 1:7,000. Fusion occurs in 85% to 90% of CRE cases. Left-to-right renal crossover is more common than right-to-left crossover.
CFRE results from abnormal embryonic kidney development. Initially, the developing kidneys are adjacent within the pelvis, with the hila facing anteriorly. As the fetus grows, the kidneys ascend into the abdomen until the ninth week of gestation, when they assume their final positions as they come in contact with the adrenal glands. During ascent, the kidneys rotate 90° medially with the superior pole oriented anteromedially and the inferior portion inferolaterally. Overrotation or lack of rotation is known as malrotation of the kidney. In CFRE, the ectopic kidney is frequently malrotated, which can contribute to urological complications such as uteropelvic obstruction, renal stones, and urinary tract infections.
Several variations in arterial supply and venous drainage have been observed in ectopic kidneys. Normally, as the developing kidneys ascend from the pelvis, they receive blood supply sequentially from the medial sacral artery, common iliac artery, inferior mesenteric artery, and finally from the aorta. In their final positions, they retain the renal arteries branching from the abdominal aorta while other previously acquired vessels degenerate. However, in the ectopic kidney, the embryonic developmental blood supply may not disappear, while the renal artery forms from one permanent branch.
Ectopic renal kidneys are differentiated based on their locations. CRE is classified into four groups: CRE with fusion (85% to 90% of CRE cases), CRE without fusion, solitary CRE, and unfused bilateral CRE (very rare). There are six subtypes of CFRE: inferior CFRE (most common), sigmoid kidney, lump kidney, disc kidney, L-shaped kidney, and superior CFRE (least common).
Renal abnormalities such as ectopia can be detected by various modalities including ultrasound, IV pyelography, CT, angiography, and MRI. CT is the best imaging modality to identify renal ectopia and associated complications.
Ultrasound is typically the first modality of imaging used during workup. Ectopia may be suspected if there is an empty renal fossa and confirmed if the ectopic kidney is located. Ultrasound findings suggestive of CFRE include an enlarged kidney (greater than 13 cm in length for an adult) and a characteristic echogenic notch seen anteriorly and/or posteriorly at the fusion site.
Symptomatic cases of CFRE may present with flank or abdominal pain, palpable mass, hematuria, dysuria, or urinary tract infection. The most common complication of CFRE is vesicoureteral reflux. Other complications include hydronephrosis, nephrolithiasis, recurrent urinary tract infections, and increased risk of infection in the case of a kidney low in the abdomen with a short ureter. Additionally, an ectopic kidney may be more prone to blunt trauma, as it may be located in a less protected space in the abdomen or pelvis outside of the perirenal capsule.
CRE can be associated with other congenital urological anomalies such as ureteral duplication, ectopic ureter, ureterocele, retrocaval ureter, cryptorchidism, hypospadias, urethral valve and cystic dysplasia in men, and unilateral agenesis of fallopian tubes and ovaries and unicornuate uterus in women. Other nonurological anomalies associated with CRE include skeletal abnormalities such as spina bifida and congenital hip dysplasia, gastrointestinal abnormalities such as imperforate anus and esophageal atresia, and cardiopulmonary abnormalities.
There is no primary treatment for CFRE, as it is largely asymptomatic. Management of CFRE depends on the presence of symptomatic complications such as obstruction, hydronephrosis, nephrolithiasis, and vesicoureteral reflux, where surgery may be needed. Extensive renal damage may warrant nephrectomy.
— Fatima Khan, BS, is a medical student at Frank H. Netter School of Medicine at Quinnipiac University.
— Daniel Chen, MD, is a radiology resident at UConn Health at the University of Connecticut.
— Marco Molina, MD, is an assistant professor of radiology at UConn Health.
Resources
1. Patel TV, Singh AK. Crossed fused ectopia of the kidneys. Kidney Int. 2008;73(5):662.
2. Hertz M, Rubinstein ZJ, Shahin N, Melzer M. Crossed renal ectopia: clinical and radiological findings in 22 cases. Clin Radiol. 1977;28(3):339-344.
3. Solanki S, Bhatnagar V, Gupta AK, Kumar R. Crossed fused renal ectopia: challenges in diagnosis and management. J Indian Assoc Pediatr Surg. 2013;18(1):7-10.
4. McDonald JH, McClellan DS. Crossed renal ectopia. Am J Surg. 1957;93(6):995-1002.
5. Muttarak M, Sriburi T. Congenital renal anomalies detected in adulthood. Biomed Imaging Interv J. 2012;8(1):e7.