 On the Case
On the Case
By Nicholas Luibil, DO; Dmitry Trifanov, MD, PhD; and Min-Chul Shin, MD
Radiology Today
Vol. 23 No. 4 P. 30
History
A 59-year-old woman presented with several months of umbilical pain and bleeding from the umbilicus which coincided with her menstrual period. She had a history of dysmenorrhea and a remote history of an umbilical hernia repair. CT imaging of the abdomen and pelvis was ordered. CT imaging was performed during the patient’s menstrual period.
Findings
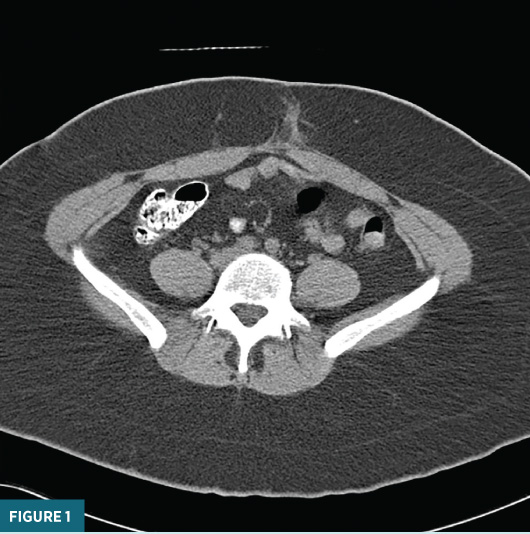
An unenhanced axial CT image inferior to the umbilicus (Figure 1) demonstrated ill-defined soft tissue inflammatory changes within the anterior abdominal subcutaneous fat.
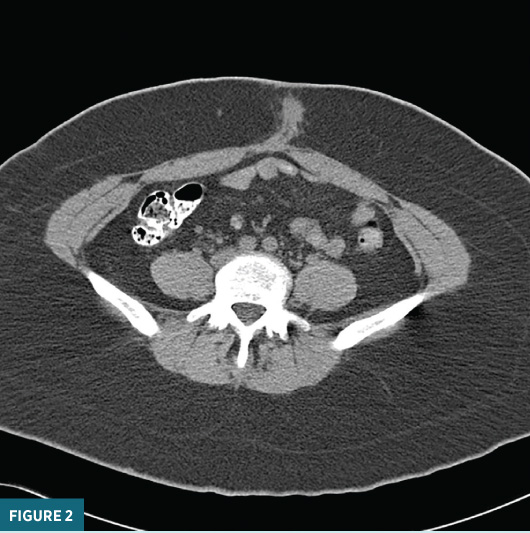
An unenhanced axial CT image slightly superior to Figure 1, and just below the level of the umbilicus (Figure 2), demonstrated a rounded soft tissue lesion in the anterior abdominal wall.
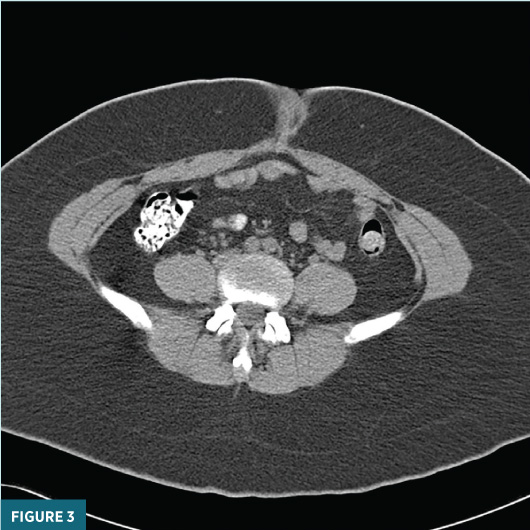
An axial unenhanced CT image at the level of the umbilicus (Figure 3) demonstrated a 3.9 cm X 3.4 cm slightly heterogenous high-attenuation umbilical lesion.
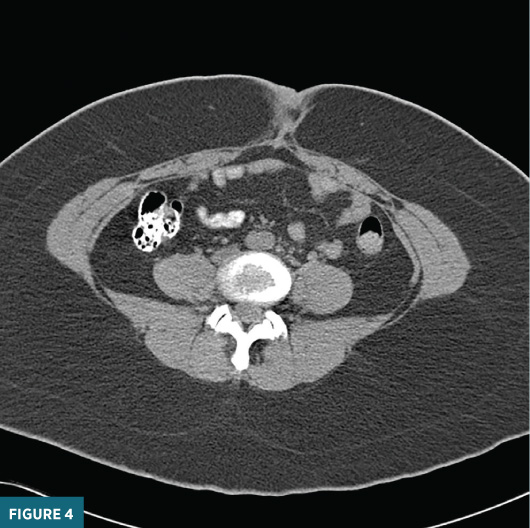
An unenhanced axial CT image at the superior aspect of the umbilicus (Figure 4) revealed a mixed soft tissue and blood attenuation.
The mass was surgically removed. Histopathology demonstrated a florid cystic and glandular proliferation within a soft tissue mass with areas of marked cellular atypia. These findings were consistent with clear cell carcinoma arising in the background of endometriosis.
Diagnosis
Endometriosis-associated clear cell carcinoma of the umbilicus.
Discussion
Endometriosis is an estrogen-dependent inflammatory condition and the leading cause of chronic pelvic pain in premenopausal women. Endometriosis occurs when endometrial tissue sheds from the uterine cavity and implants throughout the abdomen. Additional typical clinical presentations include cyclic abdominal pain coinciding with menses, infertility, and dyspareunia.1
In the vast majority of cases identified at surgery, the most commonly involved tissues include the pelvic peritoneal surfaces, rectovaginal space, and ovaries. Less commonly, endometriosis can affect the bladder, bowel, and, rarely, the abdominal wall.1 In the literature, multiple cases of abdominal wall endometriosis in surgical scars developing after cesarean section have been described, and it is hypothesized that intraoperative implantation occurs with the opening of the uterine cavity.2,3 In the exceedingly rare instance of umbilical endometriosis—which only occurs in about 0.5% to 1% of endometriosis cases—it is hypothesized that endometrial tissue may implant on umbilical scars that form after laparoscopy.4
Endometriosis at any site has an associated risk of malignancy of 1%. Of these malignant cases, 80% occur within ovarian endometriosis, or endometriomas, while 20% occur at extragonadal sites.2 Subtypes of endometrial carcinomas include endometrioid carcinoma (up to 85% of cases of endometrial carcinoma in the United States are of the endometrioid subtype), serous carcinoma, clear cell carcinoma, and carcinosarcoma.3,5,6 Clear cell carcinomas are relatively rare, contributing to only about 5% of endometrial carcinomas, but portend a poor prognosis—the five-year overall survival rate has been reported as roughly 25% to 52% in advanced-stage disease.6 The more common endometrioid subtype is associated with chronic estrogen exposure and endometrial hyperplasia, while clear cell carcinoma is not.5
Endometriosis occurring from surgical scars in the abdominal wall is a well-documented entity, with umbilical endometriosis being a relatively rare variation. This case of endometriosis-associated clear cell carcinoma of the umbilicus demonstrates that endometriosis should be in the differential diagnosis for any umbilical mass in a female, especially one presenting with cyclical pain and umbilical bleeding. Rarely, endometriosis at any site may undergo malignant transformation and therefore close monitoring for any aggressive features is prudent.
— Nicholas Luibil, DO, is a diagnostic radiology resident at ChristianaCare in Newark, Delaware.
— Dmitry Trifanov, MD, PhD, is a staff radiologist at ChristianaCare.
— Min-Chul Shin, MD, is a staff radiologist at ChristianaCare.
References
1. Bulun SE, Yilmaz BD, Sison C, et al. Endometriosis. Endocr Rev. 2019;40(4):1048-1079.
2. Carsote M, Terzea DC, Valea A, Gheorghisan-Galateanu AA. Abdominal wall endometriosis (a narrative review). Int J Med Sci. 2020;17(4):536-542.
3. Giannella L, Serri M, Maccaroni E, et al. Endometriosis-associated clear cell carcinoma of the abdominal wall after caesarean section: a case report and review of the literature. In Vivo. 2020;34(4):2147-2152.
4. Makena D, Obura T, Mutiso S, Oindi F. Umbilical endometriosis: a case series. J Med Case Rep. 2020;14(1):142.
5. Paulino E, de Melo AC, da Silva VF. Endometrioid carcinoma arising from an endometriosis-associated abdominal wall scar. Am J Case Rep. 2020;21:e922973-1-e922973-6.
6. Sun Y, Liu G. Endometriosis-associated ovarian clear cell carcinoma: a special entity? J Cancer. 2021;12(22):6773-6786.
