 January/February 2026 Issue
January/February 2026 Issue
Billing and Coding: 2026 Coding Update
By Melody W. Mulaik, MSHS, CRA, RCC, RCC-IR, FAHRA
Radiology Today
Vol. 27 No. 1 P. 26
2026 is a big year for changes in radiology for both diagnostic and interventional services. These changes may require more details in physician documentation and changes to operational workflows to ensure proper scheduling, prior authorization (for some procedures), and accurate charge capture.
The following is a high-level summary of some of the key coding changes. The CPT Manual should be reviewed in detail to ensure identification of all relevant additions, deletions, and revisions for your organization.
Lower Extremity Revascularization
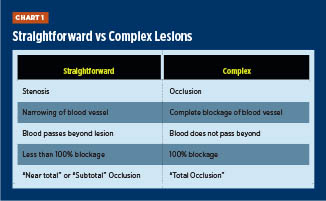
The biggest changes are in the interventional code set and, specifically, the lower extremities. Forty-six new codes for percutaneous lower extremity revascularization (37254–37299) now exist, and the previous code set (37220–37235) has been deleted for 2026. Like the now-deleted codes, the new codes are still unilateral by definition and defined by territory, but there are significant changes to the definitions. Key highlights include the addition of a new territory for procedures performed in the inframalleolar vessels, the addition of codes for intravascular lithotripsy (IVL) in the iliac and femoral/popliteal territories, and the designation of straightforward vs complex lesions.
In short, a straightforward lesion is defined as a stenosis, and a complex lesion is defined as an occlusion where there is no blood flow through the lesion. The determination of straightforward vs complex lesions is based on the status of the vessel immediately prior to the revascularization procedure. All of the codes, except for the two add-on IVL codes, are defined as either straightforward or complex so it is critical that the physician documentation clearly indicate the characteristics of the lesion. Chart 1 can assist with ensuring that lesions are classified correctly according to CPT guidelines.
Physician documentation must clearly state the exact location of performed procedures as well as the characteristics of the lesion(s) to ensure the accurate codes can be assigned. All of the new codes include catheterization of the treated vessel(s) through the same access site and all intraprocedural imaging guidance. The codes do not include intravascular ultrasound (37252–37253), diagnostic angiograms that meet coding criteria requirements, or catheterization through a different puncture site. The guidelines contained in the CPT Manual should be reviewed in detail to ensure correct assignment of the new codes.
Chart 2 shows the vascular territories, included arteries, intervention(s) covered by the new CPT codes, and the code ranges for each territory.
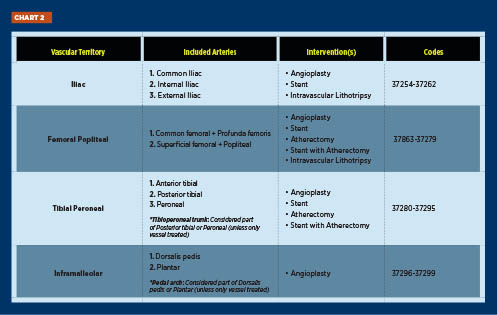
Physician documentation should clearly specify whether each lesion is straightforward or complex, identify the vascular territory and the number of vessels treated, and detail the specific intervention performed—such as angioplasty, stenting, atherectomy, or IVL—to ensure accurate code assignment. IVL addon codes should be applied only in the iliac and femoralpopliteal territories, with unlisted codes used when IVL is performed elsewhere.
Head and Neck Embolizations
Significant revisions were made to head and neck endovascular therapy embolization codes 61624 and 61626. All radiological supervision and interpretation, intraprocedural roadmapping, and imaging guidance have now been fully bundled into 61624 and 61626, eliminating the need to separately report the imaging components 75894 and 75898. While these two radiological supervision and interpretation codes still exist in the CPT Manual, there are no instances where these codes should be reported with head and neck embolization procedures. Introductory guidelines and parenthetical notes were also updated to reflect this consolidation.
Prostate Biopsies
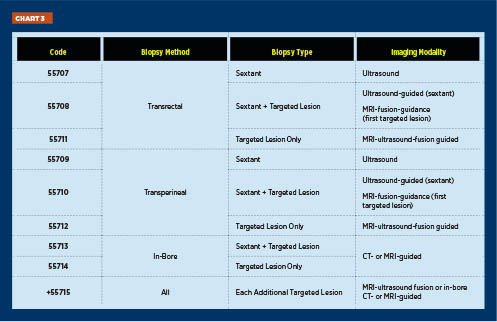
The prostate biopsy codes (Chart 3) have been updated to better define the type of imaging guidance utilized for the procedure. MRI-ultrasound fusion biopsy includes the additional work of fusing previously performed MR imaging with real-time ultrasound on an independent workstation. Image-guided targeted biopsies are reported once per lesion. While interventionalists will only do some of these procedures, it is good to know all of the available codes.
Irreversible Electroporation (IRE)
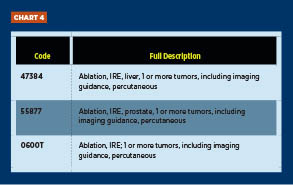
Two new codes have been added for percutaneous IRE of the liver and prostate (Chart 4). Both codes include imaging guidance. The existing category III code 0600T should continue to be reported for IRE ablation of any other organ.
Endovascular Repair of Thoracic Aortic Aneurysms
The 2026 updates to the thoracic aortic aneurysm endovascular repair codes broaden the scope of existing CPT codes by expanding their applicability from solely the descending thoracic aorta to the entire thoracic aorta. Key revisions include removing “descending” from code descriptors; bundling associated preprocedure tasks such as sizing, device selection, catheterization, and radiological supervision and interpretation; and introducing new comprehensive codes like 33882.
Several outdated codes (33844, 33889, 33891, and 75945–75959) have been deleted as part of this restructuring, while others (33880, 33881, 33883, and 33886) have been revised to reflect current procedural practice and reporting standards.
Head and Neck CT Angiography (CTA) and Cerebral Perfusion
There is a new combination code for CTA of the head and neck. See Chart 5.
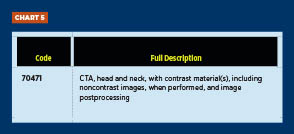
The existing codes for CTA of the head (70496) and CTA of the neck (70498) still exist and should be assigned when single studies are performed.
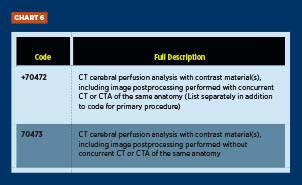
The existing Category III code for cerebral perfusion (0042T) has been deleted, and two new codes have been created to report CT cerebral perfusion. The add-on code 70472 should be assigned when performed in conjunction with CT or CTA of the head. See Chart 6.
Quantification and Characterization of Coronary Atherosclerotic Plaque
The Category III codes 0623T–0626T for automated quantification and characterization of coronary atherosclerotic plaque have been deleted and replaced with the new category I code 75577. See Chart 7.
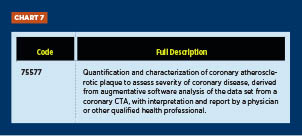
Code 75577 is reported once per coronary CTA and does not include interpretation and reporting of coronary CTA (75574).
Summary
As we continue to implement the 2026 updates, it’s important to remember that procedure codes directly translate into reimbursement, affecting both our patients and our providers. The new codes are already driving changes in workflows and requiring additional education for our physicians, technologists, coders, and other staff to ensure accurate and consistent code assignment. By working together and keeping all stakeholders engaged as these updates roll out, we can provide the support needed to achieve smooth, organizationwide adoption.
— Melody W. Mulaik, MSHS, CRA, RCC, RCC-IR, FAHRA, is the chief operations officer of R3: Powering RCCS, Regents Health Resources, and RC Billing.
DISCLAIMER: CPT is a registered trademark of the American Medical Association. CPT five-digit codes, nomenclature, and other data are copyright 2025 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative values, or related listings are included in the CPT book. AMA does not directly or indirectly practice medicine or dispense medical services. AMA assumes no liability for the data contained herein or not contained herein.
