History
A 27-year-old male with no significant past medical history was brought to the emergency department after being found unresponsive. On arrival, the patient was toxic-appearing, diaphoretic, and lethargic, responding only to deep sternal rub. Mental status improved following the administration of 1 mg of naloxone. A urine toxicology screen was positive for cocaine and cannabinoids, and the patient subsequently admitted to recent inhalation of crack cocaine. A chest radiograph and chest CT were obtained, and the patient was admitted for continued stabilization.
Findings
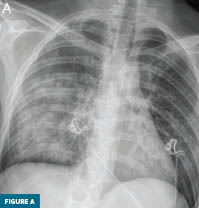
Figure A: Anteroposterior chest radiograph demonstrates diffuse airspace opacity throughout the right mid and lower lung zones.
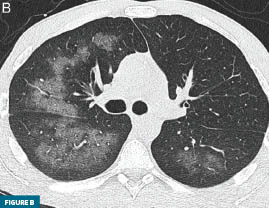
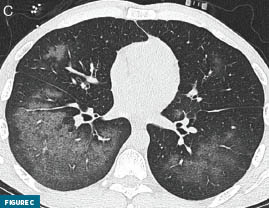
Figures B and C: Axial chest CT images with lung windowing demonstrate diffuse multilobar ground-glass opacities with peripheral sparing, most prominent in the right lower lobe.
During the admission, the patient was managed with supplemental oxygen, continuous cardiorespiratory monitoring, and bronchodilator therapy. Empiric broad-spectrum antibiotics were initiated given the radiographic appearance, which raised concern for bacterial pneumonia; the antibiotics were deescalated following the return of negative infectious cultures. The patient’s respiratory status improved progressively, with symptom resolution occurring within 48 to 72 hours of cocaine cessation and supportive management. He was discharged in stable condition with substance use counseling arranged at follow-up.
Diagnosis
Cocaine-induced acute pulmonary injury, colloquially known as “crack lung.”
Discussion
The pathophysiology of crack lung is multifactorial. The high temperature of inhaled crack cocaine smoke and its combustion byproducts cause caustic thermal and chemical injury to the alveolar-capillary membrane, resulting in increased membrane permeability and noncardiogenic pulmonary edema. Cocaine’s sympathomimetic properties produce pulmonary vasoconstriction, leading to ischemic injury followed by reperfusion injury as the drug is cleared. Simultaneously, cocaine triggers a robust immunological and inflammatory response characterized by an influx of eosinophils and cytokines into the alveolar spaces, causing diffuse alveolar damage and hemorrhage. Bronchoalveolar lavage fluid may demonstrate black pigmented macrophages or hemosiderin-laden macrophages, hallmarks of smoke inhalation and alveolar hemorrhage.1,2
On chest radiograph, crack lung typically presents with acute-onset bilateral airspace opacities that may mimic pulmonary edema or pneumonia. However, as illustrated in this case, an asymmetric or predominantly unilateral distribution may be encountered, particularly early in the clinical course. On chest CT, crack lung characteristically demonstrates diffuse multilobar ground-glass opacities with smooth interlobular septal thickening and areas of consolidation representing diffuse alveolar damage or hemorrhage.3,4
Management is primarily supportive, centered on cocaine cessation and supplemental oxygen. Mechanical ventilation may be required in cases of severe hypoxemia. Corticosteroid therapy is effective when a significant eosinophilic or inflammatory component is present, and bronchodilators may be used for symptomatic relief. Because the radiographic presentation can closely mimic bacterial pneumonia, empiric broad-spectrum antibiotics are commonly initiated at admission and de-escalated once infectious cultures return negative.1,2 The prognosis is generally favorable, with symptoms typically resolving within 48 to 72 hours of drug cessation and supportive therapy. Recurrent exposure carries a risk of progressive chronic interstitial lung disease and pulmonary fibrosis.2
Crack lung represents an underrecognized but important form of acute pulmonary toxicity that warrants a place in the radiologist’s differential diagnosis. In any patient with a known or suspected history of cocaine use presenting with acute hypoxemia and diffuse airspace opacities, this diagnosis should be actively considered. A thorough drug-use history is essential, as the diagnosis is fundamentally clinical and radiographic confirmation is nonspecific. Early recognition enables prompt initiation of appropriate supportive care, avoids unnecessary diagnostic delay, and—as this case illustrates—informs a rational de-escalation strategy when infectious cultures return negative.
— Sharon Lee, DO, is a radiology resident at AdventHealth Orlando in Florida.
— Darel Heitkamp, MD, is a cardiothoracic radiologist at AdventHealth and an affiliate professor of radiology at the University of Central Florida College of Medicine.
References
1. Centers for Disease Control and Prevention. Acute lower respiratory tract illness in illicit drug users—South Carolina, 1995. MMWR Morb Mortal Wkly Rep. 1995;44(39):727, 733-734.
2. Giacomi FD, Srivali N. Cocaine use and crack lung syndrome. QJM. 2019;112(2):125-126.
3. Restrepo CS, Carrillo JA, Martínez S, Ojeda P, Rivera AL, Hatta A. Pulmonary complications from cocaine and cocaine-based substances: imaging manifestations. Radiographics. 2007;27(4):941-956.
4. Roset-Altadill A, Wat D, Radike M. Cardiovascular and pulmonary complications of recreational drugs: a pictorial review. Eur J Radiol. 2024;178:111648.