 On the Case
On the Case
By Youssef Beshay, MD; Victoria Abalyan, BS; and Alex Merkulov, MD
Radiology Today
Vol. 26 No. 8 P. 30
History
A 39-year-old male with no significant past medical history presented to the emergency department (ED) with a two-day history of sharp, stabbing, right-sided chest pain associated with mild shortness of breath. The pain was pleuritic in nature—worsening with deep inspiration and changes in position. The patient also reported lightheadedness, decreased oral intake, and a two-week history of nausea, vomiting, and diarrhea without accompanying abdominal pain. He denied fever, chills, hematemesis, melena, or hematochezia.
The patient reported recent upper respiratory symptoms with nasal congestion approximately two weeks prior but denied cough, hemoptysis, or recent travel. There was no history of deep venous thrombosis, pulmonary embolism, or prolonged immobilization. He denied tobacco use and stated that he had stopped smoking marijuana three to four weeks prior.
The patient described a decline in appetite, unintentional weight loss, and general malaise over the preceding several weeks. He is typically physically active and exercises regularly.
ED point-of-care ultrasound demonstrated a large, right atrial mass, and a CT angiography of the chest was ordered.
Findings
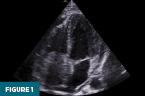
Frontal and lateral chest radiographs demonstrated a mildly prominent cardiac silhouette. Point-of-care echocardiography in the apical four-chamber view revealed an echogenic mass occupying much of the right atrium (Figure 1).
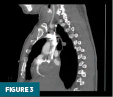
CT pulmonary angiography demonstrated a heterogeneous, lobulated softtissue mass centered within the right atrium, measuring approximately 6.0 × 7.3 × 5.2 cm. The mass caused inferior displacement of the tricuspid valve and leftward deviation of the interatrial septum. A small pericardial effusion was also present (Figures 2 and 3).

Concurrent abdominopelvic CT revealed distension of the inferior vena cava (IVC) with heterogeneous enhancement, suspicious for tumor extension into the IVC (Figures 4 and 5).


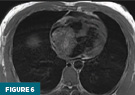
Cardiac MRI performed with and without intravenous contrast showed a heterogeneous right atrial mass nearly filling the atrial cavity. The lesion had a broad-based attachment to the interatrial septum. Punctate foci of intrinsic T1 hyperintensity suggested internal hemorrhage or necrosis. Perfusion and delayed-enhancement sequences demonstrated mild heterogeneous enhancement (Figures 6–9).



The imaging constellation was most consistent with a primary cardiac neoplasm, with differential considerations including myxoma and angiosarcoma. Metastatic disease—such as melanoma— was also considered, though there was no known history of a primary malignancy. The enhancement pattern and heterogeneity made thrombus significantly less likely.
During intensive care monitoring, the patient developed acute hypoxia and was found to have new bilateral pulmonary emboli with large occlusive and nonocclusive clot burden and signs of right-heart strain. The etiology of the emboli—bland thrombus vs tumor emboli—was uncertain. Because of worsening hypoxic respiratory failure and cardiogenic shock, the patient was transferred to a tertiary center where he underwent right atrial tumor resection, biopsy of epicardial nodules, bilateral pulmonary embolectomy, and resection of tumor thrombus from the IVC. Residual tumor infiltrating the interatrial septum and right inferior pulmonary vein was not resected. Histopathologic evaluation with immunohistochemical staining confirmed the diagnosis of angiosarcoma.
Following surgery, the patient was managed by oncology. Radiation therapy was not pursued given the extensive endocardial and epicardial involvement. Systemic chemotherapy with the AIM (Adriamycin, Ifosfamide, and Mesna) regimen was initiated, with plans to transition to taxanebased or immunotherapy regimens as indicated. Ongoing surveillance with follow-up cardiac MRI was planned.
Diagnosis
Primary cardiac angiosarcoma
Discussion
Primary cardiac angiosarcoma is a rare, highly aggressive malignant tumor arising from endothelial cells lining the blood vessels of the heart. Primary cardiac tumors themselves are extremely uncommon, with an estimated prevalence of 0.001% to 0.03%, and only about one-quarter of these are malignant. Of the malignant cardiac neoplasms, angiosarcoma accounts for approximately 30%. The tumor most frequently originates in the right atrium and often extends to involve the pericardium. Rapid proliferation of abnormal vascular channels leads to myocardial invasion, destruction of normal cardiac tissue, and local as well as distant spread, contributing to its poor prognosis.
Cardiac angiosarcoma demonstrates a male predominance (2 to 3:1) and typically occurs in individuals younger than 65 years. Because of its rapid growth and tendency for early metastasis—most often to the lungs, liver, and lymph nodes— many patients present with advanced disease at diagnosis. Reported five-year survival rates are approximately 14%.
Symptoms depend on tumor size, location, and degree of cardiac or systemic involvement. Dyspnea is the most common presenting symptom, often related to obstruction of intracardiac blood flow and subsequent heart failure. Other clinical manifestations include pericardial effusion, cardiac tamponade, chest pain, fatigue, palpitations, and syncope. Systemic or constitutional symptoms such as weight loss, anemia, and malaise may also be present.
Definitive diagnosis requires histopathologic confirmation through surgical resection or open cardiac biopsy; however, imaging plays a central role in detection, characterization, and staging.
Echocardiography is typically the first-line imaging modality. Both transthoracic echocardiography (TTE) and transesophageal echocardiography can identify tumor location, size, mobility, and hemodynamic impact. On TTE, angiosarcomas usually appear as irregular, broad-based, infiltrative right atrial masses with limited mobility and evidence of myocardial invasion.
CT provides improved anatomic definition and allows evaluation for extracardiac extension or systemic metastases. On CT, angiosarcomas often appear as low-attenuation, irregular, or nodular right atrial masses with areas of central necrosis and heterogeneous enhancement. Infiltrative pericardial thickening or effusion may be present due to hemorrhagic tumor debris.
Cardiac MRI offers superior soft-tissue contrast and detailed evaluation of local tumor extent. These lesions typically show heterogeneous signal intensity with mixed high and intermediate signal on both T1- and T2-weighted sequences, due to intralesional hemorrhage and necrosis. Focal or peripheral areas of T1 hyperintensity correspond to blood products. On contrast-enhanced images, variable heterogeneous enhancement is typical and, in cases of diffuse pericardial infiltration, linear enhancement along vascular channels may produce a “sunray” appearance. The high vascularity of these tumors leads to prominent enhancement on perfusion and delayed-phase sequences.
The differential for an intracardiac right atrial mass is broad and includes thrombus, metastasis, myxoma, lipoma, osteosarcoma, leiomyosarcoma, primary cardiac lymphoma, and undifferentiated sarcoma.
Thrombus typically lacks contrast enhancement and is associated with atrial fibrillation or low-flow states.
Myxoma is usually benign, located in the left atrium, and demonstrates a mobile, pedunculated morphology attached to the interatrial septum.
Lipoma appears as a homogeneous low-attenuation mass on CT with high T1 signal suppressed on fat-saturated MRI sequences.
Osteosarcoma and leiomyosarcoma tend to arise from the left atrium, with the former often demonstrating calcifications.
Primary cardiac lymphoma occurs primarily in immunocompromised individuals, presenting as a mass or diffuse pericardial involvement.
Undifferentiated pleomorphic sarcoma is also more common in the left atrium and may appear as an irregular or polypoid mass.
Surgical resection remains the cornerstone of therapy and provides the best opportunity for prolonged survival, although complete excision is rarely feasible due to local invasion. Adjuvant chemotherapy and radiation are commonly used following surgery. When complete resection is not possible, radiation therapy may serve as a primary treatment option. Despite multimodal therapy, prognosis remains poor due to the tumor’s infiltrative nature, high recurrence rate, and early metastatic spread.
Primary cardiac angiosarcoma is a rare but critical diagnostic consideration in patients presenting with unexplained right-sided cardiac masses, pericardial effusion, or signs of right heart failure. Its characteristic imaging features—heterogeneous enhancement, right atrial predilection, and evidence of myocardial invasion—are key to differentiation from other intracardiac entities. Early multimodality imaging and tissue diagnosis are essential for timely management and guiding surgical and oncologic intervention.
Youssef Beshay, MD, is a radiology resident at UConn Health at the University of Connecticut.
Victoria Abalyan, BS, is a medical student at the University of Connecticut School of Medicine.
Alex Merkulov, MD, is an associate professor of radiology at UConn Health.
Resources
1. Chen Y, Li Y, Zhang N, et al. Clinical and imaging features of primary cardiac angiosarcoma. Diagnostics (Basel). 2020;10(10):776.
2. Kumari N, Bhandari S, Ishfaq A, et al. Primary cardiac angiosarcoma: a review. Cureus. 2023;15(7):e41947.
3. Araoz PA, Eklund HE, Welch TJ, Breen JF. CT and MR imaging of primary cardiac malignancies. Radiographics. 1999;19(6):1421-1434.
4. Linfeng Q, Xingjie X, Henry D, Zhedong W, Hongfei X, Haige Z. Cardiac angiosarcoma: a case report and review of current treatment. Medicine (Baltimore). 2019;98(49):e18193.
5. Bhaludin BN, Thway K, Adejolu M, et al. Imaging features of primary sites and metastatic patterns of angiosarcoma. Insights Imaging. 2021;12(1):189.