By Rahul V. Pawar, MD
History
A 34-year-old man with chronic hearing loss (since childhood) reported progressive headaches and intermittent dizziness. As part of a more comprehensive workup, he was referred for outpatient MRI.
Findings
A brain and internal auditory canal protocol was utilized given history of chronic hearing loss and dizziness. No prior studies were available for correlation.
Pertinent negatives: Based on diffusion weighted imaging and susceptibility weighted imaging, there was neither evidence of an acute/subacute infarct, nor intracranial hemorrhage, respectively. The ventricular system was within normal limits. No mass effect, shift, or herniation syndromes were present.
Nonspecific white matter signal changes were noted upon the FLAIR (fluid-attenuated inversion recovery) sequence in a clustered, bifrontal distribution that could reflect stigmata of vasospastic phenomenon (eg, migraines).
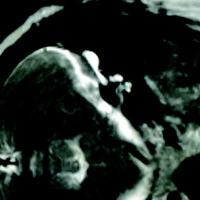
Balanced fast field echo imaging through the posterior fossa revealed T2 hyperintense varicose “cystic” spaces immediately dorsal to the semicircular canals bilaterally. The vestibular apparati seemed fairly unremarkable on both sides, as did cranial nerves VII and VIII. Upon closer inspection, however, the cochlear formations did not seem entirely normal (eg, somewhat bulbous, amorphous).
Diagnosis
Enlarged vestibular aqueduct syndrome (EVAS).
Discussion
According to the literature, EVAS is the most common imaging abnormality seen with pediatric sensorineural hearing loss (SNHL). More often than not, the condition is bilateral and hearing loss is progressive. Genetic and environmental factors have been implicated with EVAS, the common denominator being an enlarged endolymphatic sac (ES) and duct secondary to a failure of fluid absorption within the ES during embryogenesis.
Cochlear malformations are seen in a substantial number of patients with EVAS (eg, absent septation between middle and apical turns, deficient modiolus, asymmetric scalar chambers). The potentially deficient cochlea, even if functional during early childhood, is inherently vulnerable to disintegration. Even mild head trauma may ultimately lead to SNHL, though there is some phenotypic variability in this regard.
Classic MRI features include a dilated ES that may assume a varicose or beaded configuration along the posterior wall of the petrous bone. Although generally T2 hyperintense (since fluid-filled), T1 signal may vary depending on protein concentration. High-resolution temporal bone CT will demonstrate enlargement of the vestibular aqueduct +/- variable cochlear deficiencies. As mentioned above, in most cases EVAS is bilateral.
Radiologic diagnosis of EVAS at an early age may help prevent progressive deterioration of cochlear function. Avoidance of contact sports (eg, football, ice hockey) during childhood is the prevailing recommendation. Cochlear implantation can be an effective treatment for children with profound SNHL. In a review of 23 patients with EVAS published in Laryngoscope, Lee et al concluded that children did well both audiometrically and functionally after cochlear implantation.
— Rahul V. Pawar, MD, Department of Radiology, Division of Neuroradiology, is Clinical Assistant Professor, UMDNJ—New Jersey Medical School.
 |  |
| Figure 1 | Figure 2 |
References
- Davidson HC, Harnsberger HR, Lemmerling MM, et al. MR evaluation of vestibulocochlear anomalies associated with large endolymphatic duct and sac. AJNR Am J Neuroradiol. 1999;20(8):1435-1441.
- Lee KH, Lee J, Isaacson B, Kutz JW, Roland PS. Cochlear implantation in children with enlarged vestibular aqueduct. Laryngoscope. 2010;120(8):1675-1681.
- Robson CD. Large vestibular aqueduct. In: Harnsberger HR, Glastonbury CM, Michel MA, Koch BL, eds. Diagnostic Imaging: Head and Neck. 2nd ed. Salt Lake City, UT: Amirsys; 2011;VI:4:14-17.
- STATdx website. https://www.statdx.com/