By Alex King, MD
History
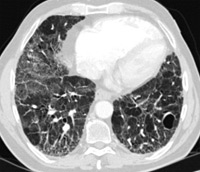
73-year-old man with 50 pack-year smoking history, progressive dyspnea, and nonproductive cough
Diagnosis
Idiopathic pulmonary fibrosis (IPF)1
Clinical
Patients are generally older than 50, with long-standing respiratory disease.
Progressive nonproductive cough and dyspnea; smoking may contribute to pathogenesis of IPF.
Median survival: two to four years; poorer prognosis compared with other interstitial lung diseases (eg, nonspecific interstitial pneumonia, respiratory bronchiolitis-associated interstitial lung disease, desquamative interstitial pneumonia).
Key Diagnostic Features (High-Resolution CT)
Low lung volumes, subpleural reticular opacities, macrocystic honeycombing ,and traction bronchiectasis
Basilar predominance (apicobasal gradient)
Characteristic features and appropriate clinical history obviates need for biopsy: High-resolution CT pattern is virtually diagnostic. (For more information, reference ATS/ERS Multidisciplinary Consensus Statement regarding the major and minor criteria for establishing diagnosis of IPF without lung biopsy.)
Differential Diagnosis
Important to exclude potential underlying causes of pulmonary fibrosis (eg, asbestos exposure, drugs, connective tissue disorders).
Treatment
Does not respond to high-dose steroids; might even be contraindicated.
Early diagnosis warrants consideration for lung transplantation.
 |
 |
| Slide 1 | Slide 2 |
REFERENCES
- Mueller-Mang C, Grosse C, Schmid K, Stiebellehner L, Bankier AA. What every radiologist should know about idiopathic interstitial pneumonias. Radiographics. 2007;27(3):595-615.
Submission Instructions
Submit cases directly to Rahul V. Pawar, MD, DABR (section editor for “On the Case”) at rvp325@yahoo.com. Cases submitted should be relevant and interesting. All modalities and subspecialties within radiology are equally considered.
Case submission entails two PowerPoint slides:
SLIDE 1
a. History (one-line phrase)
b. Two to five high-quality images in JPEG format without annotations
c. Name(s) of the author(s) (three maximum) and respective institutions
SLIDE 2
a. Diagnosis
b. Concise bulleted discussion (one to two lines each), including the following: pertinent clinical history, diagnostic imaging findings, differential diagnoses, treatment (if applicable)
c. Two to three relevant and current references, preferably citing peer-reviewed radiology literature
Department of Radiology, Division of Neuroradiology
Saint Barnabas Medical Center/Barnabas Ambulatory Care Center