By Pedram Parva, MD
History
A 56-year-old woman presented with chronic back pain.
Findings
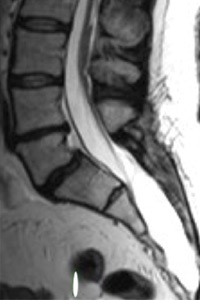
Figures A (sagittal T1) and B (sagittal T2) show low-lying conus medullaris and a small intradural lipoma (at the level of L3-L4) as well as a sacral meningeal cyst.
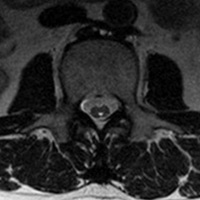
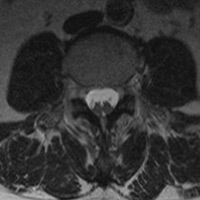
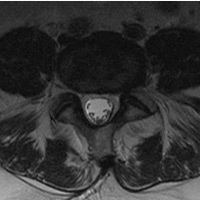
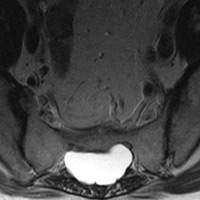
Figure C (axial T2) shows a syringomyelia (at the level of L2), and Figure D (axial T2) shows diastematomyelia (at the level of L4). Figure E (axial T2) shows a thickened filum (at the level of L4-L5) as well as a sacral meningeal cyst, in Figure F.
Diagnosis
Tethered cord syndrome
Discussion
• Tethered cord syndrome is defined as a spectrum of congenital anomalies resulting in an abnormally low position of the conus medullaris that may lead to neurological, musculoskeletal, urological, or gastrointestinal abnormalities.
• Clinical presentation in adults includes lower extremity nondermatomal pain, often referred to the anorectal region; urinary and bowel movement disorders; spastic gait; and muscle atrophy. It may be subclinical until aggravated by factors that increase tension, such as trauma, disc herniation, or spinal canal stenosis.
• MRI is the modality of choice for diagnosis. The most common findings in adults are low-lying conus (below L2 vertebra) with intra- or extradural lipoma and a short, thickened filum terminale greater than 2 mm in diameter. Less common findings are split cord malformation and a dermal sinus. CT and plain X-rays are helpful for the evaluation of scoliosis in adolescents.
• Differential diagnosis are (not limited to) degenerative joint disease, spinal cord tumor, syringomyelia, and cord compression.
• Treatment mainly is surgical, especially when the patient presents with neurological deterioration.
— Pedram Parva, MD, is an attending radiologist at the Boston University School of Medicine and the VA Healthcare System in Boston as well as a radiology instructor at Harvard Medical School.
 |
 |
| Figure A | Figure B |
 |
 |
| Figure C | Figure D |
 |
 |
| Figure E | Figure F |
- Hertzler DA Jr, DePowell JJ, Stevenson CB, Mangano FT. Tethered cord syndrome: a review of the literature from embryology to adult presentation. Neurosurg Focus. 2012;29(1):E1.
- Moriya J, Kakeda S, Korogi Y, Soejima Y, Urasaki E, Yokota A. An unusual case of split cord malformation. AJNR Am J Neuroradiol. 2006;27(7):1562-1564.
- Gupta SK, Khosla VK, Sharma BS, Mathuriya SN, Pathak A, Tewari MK. Tethered cord syndrome in adults. Surg Neurol. 1999;52(4):362-370.
Submission Instructions
- Cases should have clinical relevance and clear radiological findings.
- Seconds should include a title, history and course of illness, findings, diagnosis, and discussion.
- Word count should not exceed 800. At least three references are recommended.
- Cases may be submitted from any radiological subspecialty and imaging modality.
- Figures must be high-quality JPEG or TIFF images and labeled for ease of reference. Please keep images in their native format, without the addition of arrows or other means of highlighting the key findings.
Submit cases via e-mail to Rahul V. Pawar, MD, at rvp325@gmail.com or to Radiology Today at jknaub@gvpub.com.
Department of Radiology, Division of Neuroradiology
Saint Barnabas Medical Center/Barnabas Ambulatory Care Center